1944
Development of liver surface nodularity quantification program and its clinical application in nonalcoholic fatty liver disease1Medical Convergence Research Center, Iksan, Korea, Republic of
Synopsis
Non-alcoholic fatty liver disease (NAFLD) is the most common liver disease in the United States and its prevalence is reported to between 10% and 30%. NAFLD comprises a wide spectrum of liver damage, ranging from macrovesicular steatosis, inflammation, fibrosis, and cirrhosis. Liver biopsy has been regarded as the reference standard for diagnosing hepatic inflammation, fibrosis and cirrhosis in NAFLD. There is an unmet need for widely applicable non-invasive methods to diagnose advanced liver fibrosis and cirrhosis. Recently, liver surface nodularity (LSN) based on CT images is used to diagnose and stage a variety of liver disease in chronic liver disease, and is predictive of cirrhosis decompensation and death. The liver morphological changes in relation to fibrosis stage in NAFLD have not yet been clearly identified. Our study developed a MRI-suitable LSN quantification program and compared the fibrosis grades in NAFLD.
Introduction
Liver biopsy has been regarded as the reference standard for diagnosing hepatic inflammation, fibrosis and cirrhosis in NAFLD. There is an unmet need for widely applicable non-invasive methods to diagnose advanced liver fibrosis and cirrhosis. Instead of liver biopsy, liver MRI has great merits for screening and staging the NAFLD patients with advanced fibrosis and cirrhosis because the imaging modality is widely available (morphology, elastography, diffusion-weighted imaging, perfusion and etc) and no ionizing radiation to patients. Recently, liver surface nodularity (LSN) based on CT images is used to diagnose and stage a variety of liver disease including chronic liver disease, progressively increases with higher clinical stages of chronic liver disease and cirrhosis, and is predictive of cirrhosis decompensation and death. The liver morphological changes in relation to fibrosis stage in NAFLD have not yet been clearly identified. This study was to develop a MRI-suitable LSN software and to compare the fibrosis grades in simple steatosis (SS) and nonalcoholic steatohepatitis (NASH) based on LSN score.
Subjects and Methods
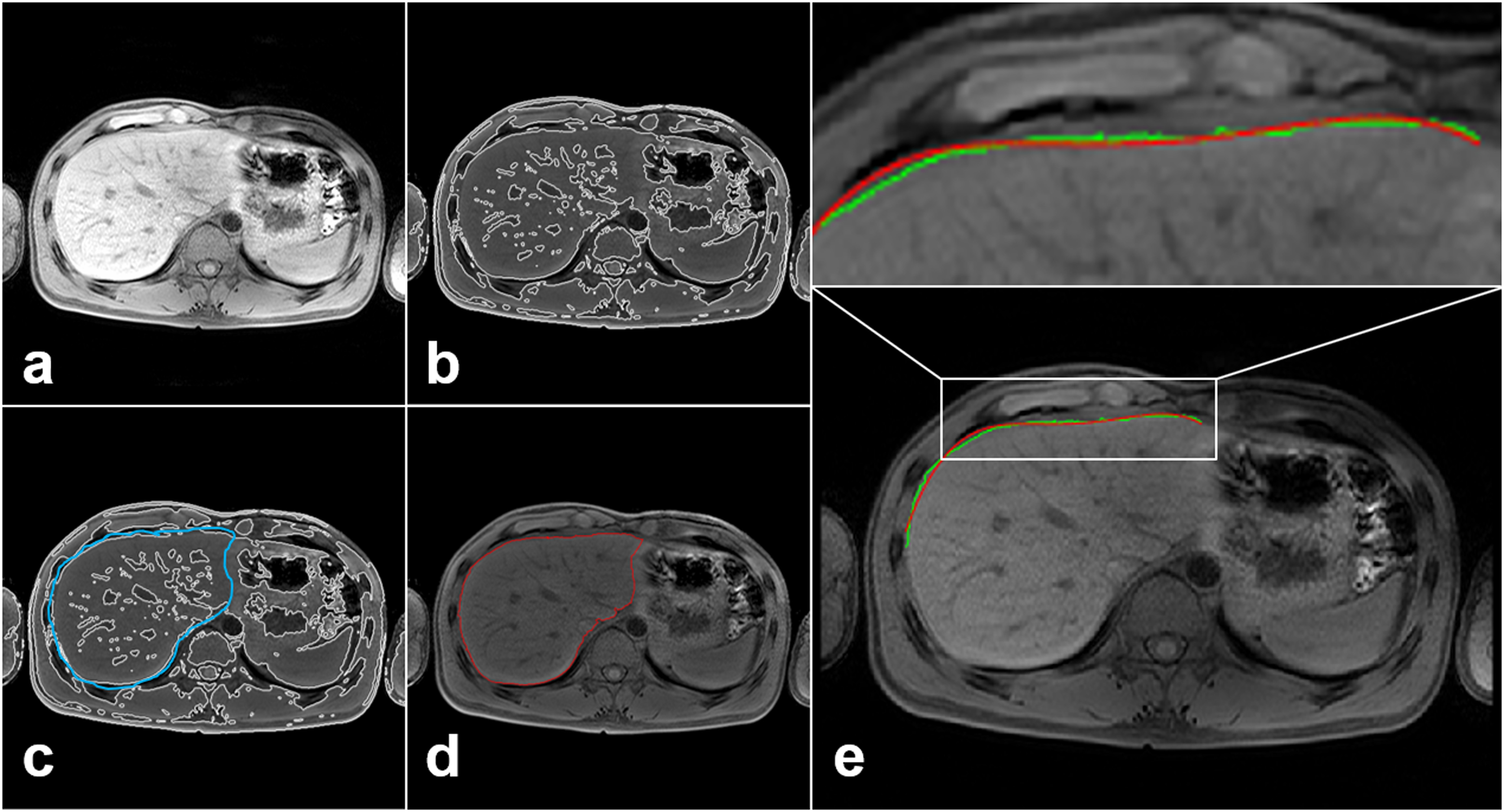
LSN program was coded by MATLAB. The LSN quantification procedure was as follows: bias correction, liver boundary detection, liver segmentation and LSN measurement (Fig. 1). A total of 30 subjects divided to three groups, consisting of 7 normal controls(NC; mean age 33.3±8.0 yrs), 12 SS (mean age 41.8±11.2 yrs) and 11 NASH (39.1±13.8 yrs). A normal control group was defined as <5% liver fat content on 1H MR spectroscopy (MRS) and NAFLD was defined as >5% liver fat content. This study was used NAFLD activity scores (NAS) based on pathology assessment. The subgroup of NAFLD is defined SS and NASH as follows: NAS <5 for SS and NAS ≥5 for NASH.
All MRI examinations were performed on a 3T MRI scanner (Achieva; Philips, Netherlands) with a 32-channel receiver body matrix coil. The T1WI (repetition time [TR]/TE= 4.2/1.97 ms) were acquired with three-dimensional T1 high-resolution isotropic volume excitation pulse sequence: field of view (FOV)= 38×38×14 cm3, matrix size= 512×512, number of excitation (NEX)= 2, slice thickness= 0.74×0.74×2.0 mm3, number of slices= 70 and scan time= 14 sec. Together with a single breath-hold technique, the imaging plane in the upper abdomen was axial and the sequence was triggered to expiration. Additional multislice T1- and T2-weighted sequences were obtained in sagittal, axial and coronal planes as the liver MRI protocol for evaluating the NAFLD. Total examination time ranged from 35–45 minutes.
LSN scores among three groups and fibrosis grades were compared using Kruskal–Wallis H test and Mann–Whitney’s post-hoc tests. Diagnostic accuracy was determined by calculating the area under the receiver operating characteristics (ROC) curve. To identify the reliability of LSN measurements in the different ROIs, coefficient of variance (CV) was calculated overall CV values for the variability of measurements. Interobserver agreement and reliability were estimated by calculating the intraclass correlation coefficient (ICC).
Results and Discussion
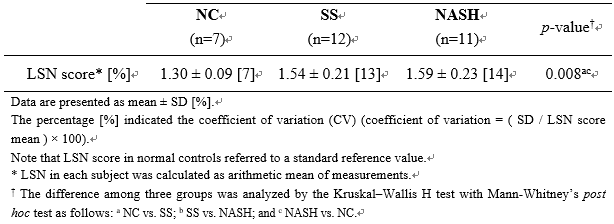
The variations of all LSN measurements are not exceeded 15%, as a mean CV value 11.3%. ICCs were higher than 0.6. The liver surface line for LSN quantification was extracted as a reference line and two radiologists (with more than 20 years of experience) finally confirmed the liver surface line (Fig. 1). Mean LSN scores in three groups were NC 1.30±0.09, SS 1.54±0.21 and NASH 1.59±0.23 (p=0.008; Table 1). Two patient groups (SS and NASH) showed higher surface nodularity scores compared to a NC group (p<0.01). However, there was not significant difference between SS and NASH patient groups (p=0.758). Therefore, the LSN quantification might be difficult to differentiate NASH (induced by hepatocellular inflammation) from simple steatosis (fat accumulation in hepatocyte).
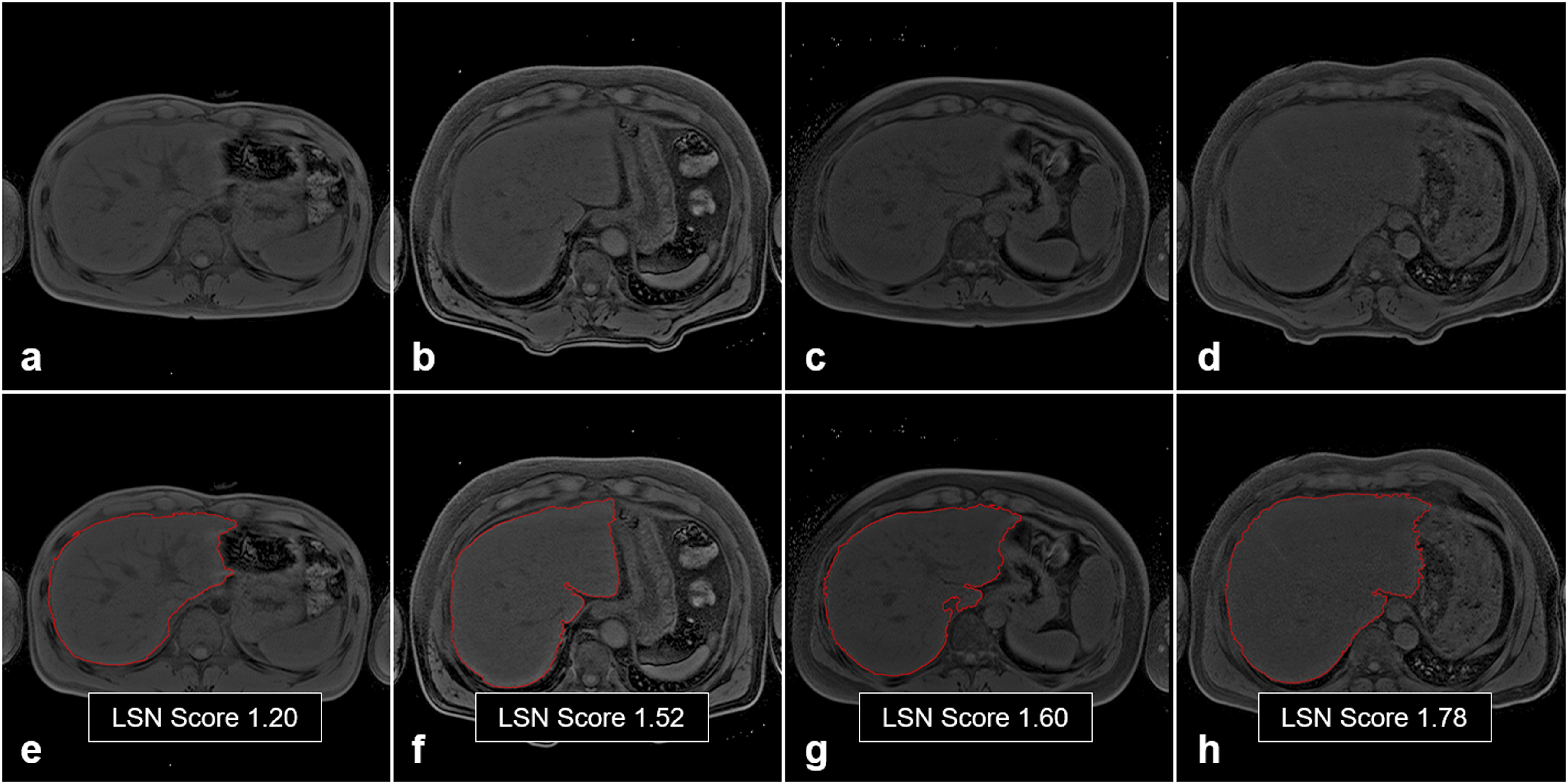
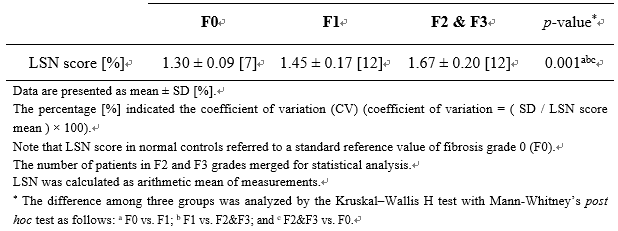
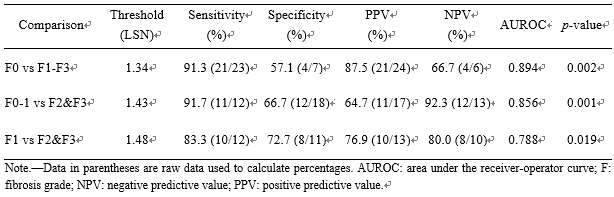
Representative LSN quantification images according to fibrosis grades (F0-F3) in Fig. 2. Mean LSN scores according to fibrosis grade (F) were F0 1.30±0.09, F1 1.45±0.17 and F2&F3 1.67±0.20 (p=0.001; Table 2). The mean LSN score in F2&F3 is significantly higher than that in F1 (p=0.019). The AUROC analysis (Table 3) to distinguish F1 and F2&F3 was 0.788 (95% CI 0.595–0.981, p=0.019) at a cut-off LSN score greater than 1.48, and its diagnostic accuracy had 0.833 sensitivity and 0.727 specificity. Thus, the LSN quantification can be a non-invasive technique capable of detecting fibrotic changes in the liver of NAFLD, and moreover, our data focusing on fibrosis grades of NAFLD can provide the evidence that liver surface nodularity is a useful quantitative imaging biomarker that can be used to diagnose and stage hepatic fibrosis.
Conclusion
This study developed MRI-suitable LSN quantification program and the LSN measurement is reproducible when applied to axial MR images in assessing fibrosis stage. The finding demonstrates that the quantitative LSN scores can help to differentially diagnose fibrosis stage in NAFLD.Acknowledgements
This study was supported by the grants of the National Research Foundation of Korea (NRF) (2016M3A9A7918501) and the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare (HI18C1216).References
1. Lonardo A, et al. Hepatology 2016; 64: 1388-1389, (2016).
2. Chalasani N, et al. Hepatology 2018; 67:328-357.
3. Dyson JK, Anstee QM & McPherson S. Frontline Gastroenterol 2014; 5: 211-218.
4. Jiang H, et al. J Clin Transl Hepatol 2018; 6: 198-207.
5. Smith AD, et al. Radiology 2016; 280: 771-781.
Figures