1904
The value of three-dimensional, compressed sensing magnetic resonance urography, with and without breath-holding: comparison of acquisition time, image quality, and diagnostic performance with conventional magnetic resonance urography1Department of MRI, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2MR Collaboration, Siemens Healthcare Ltd, Beijing, China, 3MR Application Development, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
This study aimed to prospectively evaluate the feasibility of three-dimensional (3D), compressed sensing (CS) magnetic resonance urography (MRU), with and without breath-holding (BH), for shortening the acquisition time, with better image quality and diagnostic performance. Forty-five patients were enrolled. BH-CS MRU, navigator-triggered (NT) CS MRU, and conventional NT MRU were performed. Comparisons of acquisition time, image quality (sharpness of urinary tract and background suppression), and diagnostic performance were made among these three protocols. BH-CS MRU was superior to the other MRU protocols, with the shortest acquisition time and better image quality with comparable diagnostic performance.
Introduction
There are many clinical indications for imaging the urinary tract, such as suspicious urinary tract stones, tumor, hydronephrosis. Intravenous pyelography (IVP) and computed tomography urography (CTU) are commonly used and have a short examination time, but are not used in some groups, including pregnant women because of radiation exposure risk and certain patients who were allergic to iodinated contrast media. However, magnetic resonance urography (MRU) without contrast media could overcome these limitations. MRU is widely used to provide excellent anatomical and functional evaluation of the urinary tract1. However, the long acquisition time of three-dimensional (3D) MRU makes completion of the scanning challenging for patients with a full bladder. A compressed sensing (CS) accelerated MR technique has emerged, and it shows great potential for shortening the MR data acquisition time2. The purpose of this study was to prospectively evaluate the acquisition time, image quality (sharpness of urinary tract and background suppression), and diagnostic performance of breath-holding compressed sensing (BH-CS), navigator-triggered (NT) CS (NT-CS), and conventional NT (conventional NT) 3D MRU protocols.Methods
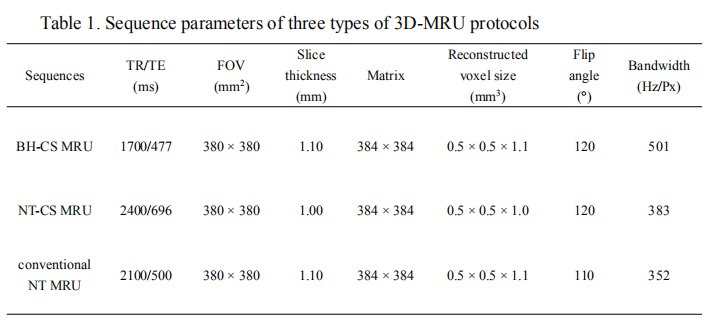
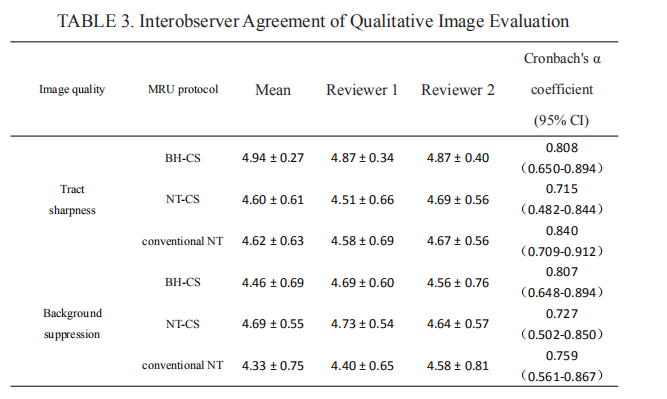
This institutional review board–approved study included 45 patients (31 men and 14 women; median age, 38 years; age range, 9 - 78 years), who underwent an MRU examination on a MAGNETOM Prisma 3 T scanner (Siemens Healthcare, Erlangen, Germany) to detect urinary system lesions. All the patients were administered furosemide intravenously (0.33mg/kg of body weight) before the MRI examination to enhance distension of the urinary tract.The MRI examination was performed using three 3D-MRU protocols, i.e. 2 prototypic CS protocols (BH-CS MRU, NT-CS MRU), and conventional NT MRU (the sequence parameters are listed in Table 1). The three protocols were performed in random order in each patient. The acquisition time of each protocol was recorded by the onsite technician. Tract sharpness and background suppression were assessed independently, based on observation of maximum intensity projection (MIP) images by two experienced radiologists, and randomly rated on a 5-point scale. Interobserver agreement was determined using Cronbach's α coefficient (< 0.50, poor; 0.51–0.70, moderate; 0.71–0.90, good; 0.91–1.00, perfect). Comparative analyses between different protocols were performed using the least significant difference or Dunnett’s T3 test, based on the homogeneity of variance. The ability of lesion detection was scored on a scale of 1 to 5 based on observation of MRU source images, MIP images, and multiplanar reconstruction (MPR) images. Sensitivity, specificity, and the AUC (area under the receiver operating characteristic (ROC) curves) were calculated based on a reference standard provided by surgical exploration, pathology results, and multimodality imaging findings. The statistical analysis was performed using SPSS 19.0 software (IBM Corp, Armonk, NY). A two-sided P-value of less than 0.05 indicated statistical significance.Results
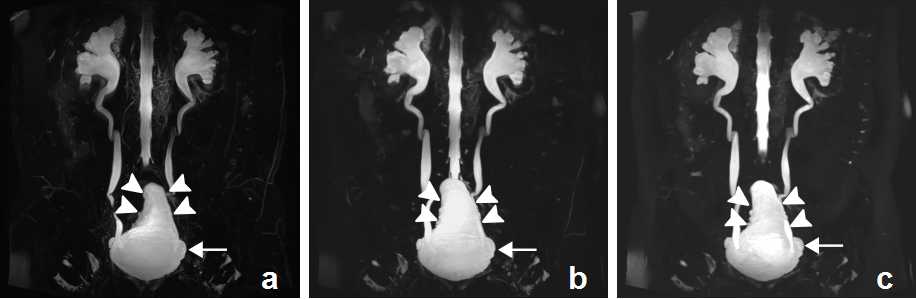
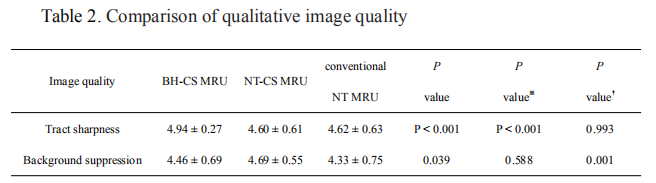
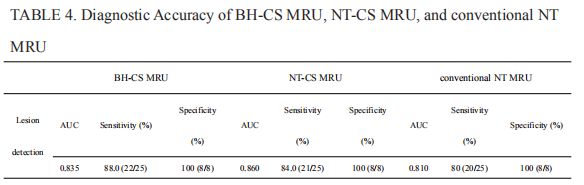
The acquisition times were 17 seconds for BH-CS MRU protocol, 206 ± 54 seconds for NT-CS MRU protocol, and 508 ± 98 seconds for conventional NT MRU protocol. BH-CS MRU protocol showed best tract sharpness with the fewest artifacts (4.94 ± 0.27) compared with NT-CS MRU (4.60 ± 0.61) and conventional NT MRU protocols (4.62 ± 0.63) (both P < 0.001) (Tables 2, 3). Background suppression for NT-CS MRU protocol (4.69 ± 0.55) was superior to BH-CS MRU protocol (4.46 ± 0.69) and conventional NT MRU protocol (4.33 ± 0.75) (P = 0.039 and P = 0.001, respectively ) (Tables 2, 3). Regarding diagnostic performance, of the 45 patients who were enrolled, only 33 matched the reference standard. Sensitivity, specificity, and the AUC value of the detection of a ureteral stricture (n = 15), stone (n = 2), horseshoe kidney (n = 1), cystitis (n = 4), and ureterocele (or renal cyst) (n = 3) were comparable for all the protocols (Table 4). A case of neurogenic bladder illustrates the typical image appearance (Figure 1).Discussion
In this study, CS-MRU protocols with and without breath-holding, and conventional NT MRU protocol, were performed in clinical patients. The acquisition time of conventional NT MRU protocol was the longest, followed by NT-CS MRU protocol and BH-CS MRU protocol. The image quality of BH-CS MRU (tract sharpness) and NT-CS MRU protocol (background suppression) was superior to that of conventional NT MRU protocol. Diagnostic efficiency was comparable among the three protocols. This may be because the shorter CS-MRU protocols should be less prone to breathing artifacts caused by discomfort from a full bladder, improving image quality, and possibly facilitating diagnostic efficiency.Conclusion
BH-CS MRU protocol is more beneficial for patients with good breath-holding ability, compared with NT-CS MRU and conventional NT MRU protocols.Acknowledgements
No acknowledgement found.References
- Morin CE, Mcbeem P, Trout AT, et al. Use of MR Urography in Pediatric Patients. Curr Urol Rep. 2018;19(11):93.2.
- Yoon JH, Yu MH, Chang W, et al. Clinical feasibility of free-breathing dynamic T1-weighted imaging with gadoxetic acid-enhanced liver magnetic resonance imaging using a combination of variable density sampling and compressed sensing. Invest Radiol 2017; 52:596-604.
Figures