1899
Impact assessment of posture and breath hold state on diaphragm shape1National Institute for Health Research (NIHR) Nottingham Biomedical Research Centre, Nottingham, United Kingdom, 2Sir Peter Mansfield Imaging Centre, University of Nottingham, Nottingham, United Kingdom, 3Respiratory Medicine, University of Nottingham, Nottingham, United Kingdom, 4School of Medicine, University of Nottingham, Nottingham, United Kingdom
Synopsis
The diaphragm plays a crucial role in respiratory mechanics. However, commonly used image acquisition methods are limited by position and breath hold duration. We developed a novel MR protocol for scanning the diaphragm in an upright low-field MR scanner and analysis tools to investigate the impact of posture and breath hold state on its morphology.
INTRODUCTION
The diaphragm is the most important muscle of respiration. Disorders of the diaphragm can have a substantial deleterious impact on respiratory function. The clinical manifestation of diaphragmatic disorders can be insidious, and underdiagnosis remains an issue. In clinical settings, pulmonary function tests, including the measurement of vital capacity in upright and supine positions, is the first-line diagnostic tools. However, although simple and inexpensive, it is effort-dependent, and does not provide anatomical details. Videofluoroscopy is also used in clinical practice to investigate diaphragmatic weakness, particularly if a unilateral disease is suspected. However, as breathing pattern changes in bilateral diaphragmatic palsy, a false negative result is possible. CT is one of the most commonly used imaging modalities used in respiratory medicine, but its role is due to the necessity of scanning patients in supine position.
The study presented here was aimed at developing and optimising novel MR imaging techniques to assess the postural change in diaphragm morphology in healthy participants using a low-field upright MR scanner.
METHODS
We scanned 10 healthy subjects (29±5 yoa) repeatedly in supine and seated position at full inspiration and full expiration (sup-exp, sup-insp, seat-exp, seat-insp) on a 0.5T Paramed MR Open (Genoa, Italy) scanner with a torso coil. A patient acceptable protocol was developed to minimise the duration of breath holds during scans. We used a 2D spin echo sequence to acquire 3 sagittal (SAG, TE/TR=12/162 ms, FA=90°, FOV=36-40 cm, matrix=256 x 256, 7-14 slices, slice thickness=10-14 mm, interslice gap=10-20 mm) and 3 coronal (COR, TE/TR=12/162 ms, FA=90°, FOV=36-40 cm, matrix=256 x 256, 7-12 slices, slice thickness=10-14 mm, interslice gap=10-14 mm) scans for each of the 4 conditions.
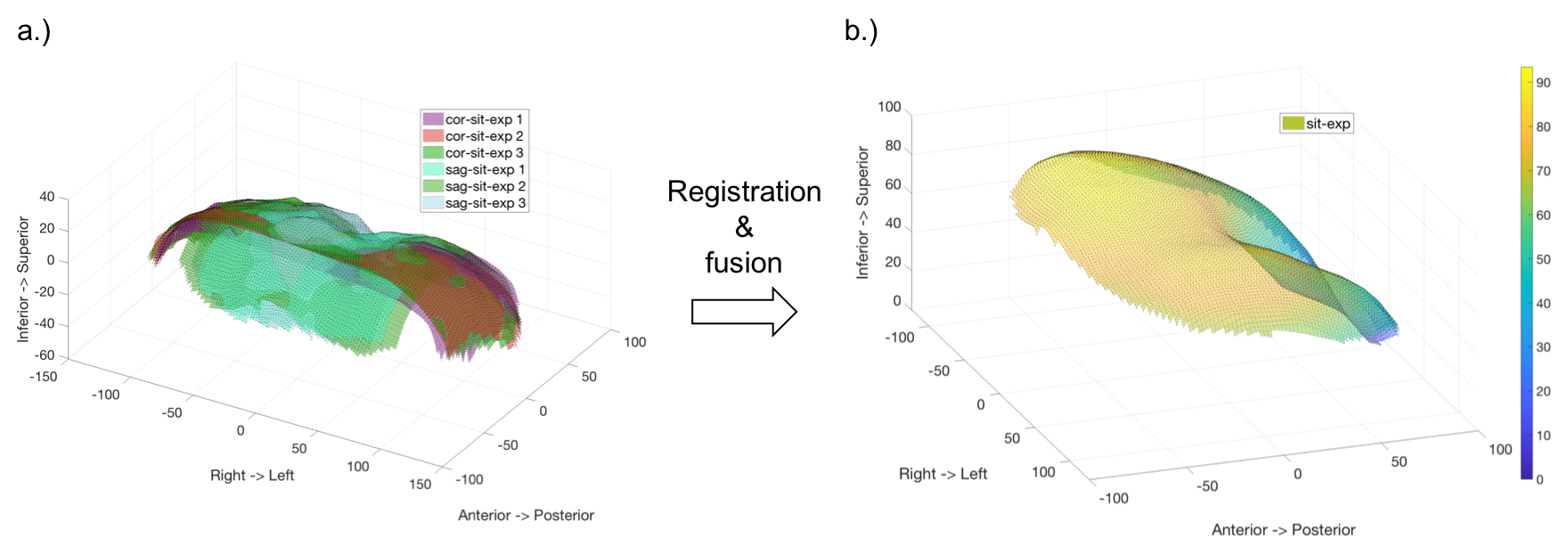
Figure 1 shows diaphragm surfaces for coronal and sagittal scans estimated from manually selected points on the diaphragm on each slice and interpolated points in between. An iterative closest point registration method was used to align all coronal and sagittal surface points and estimate a mean surface shape for each of the 4 conditions.
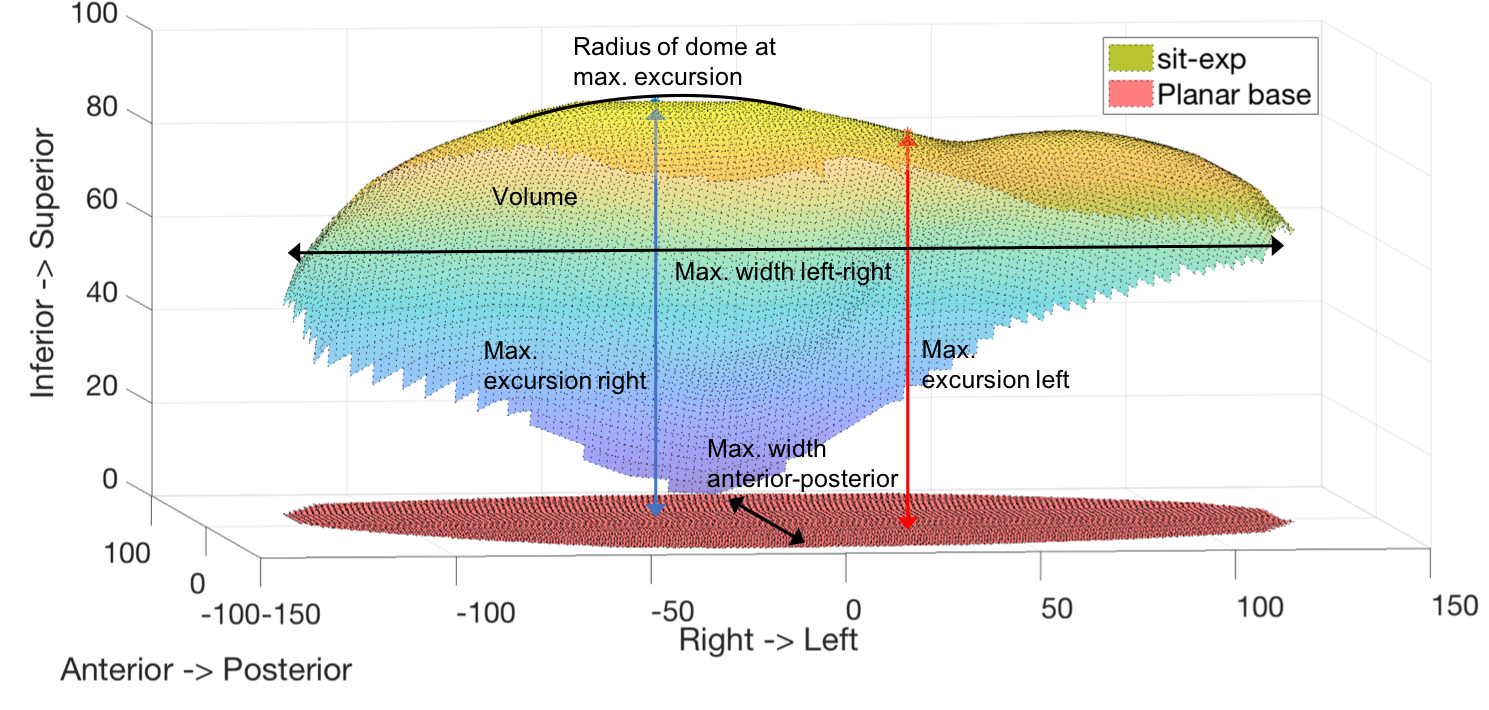
We used 6 parameters to assess the impact of the patient position and breath hold state on the diaphragm shape (Fig. 2). Parameters include the volume between the mean surface and a planar surface spanned at the most inferior point of the mean surface, the maximum excursion between mean surface and planar surface for the left and right half, the width of the diaphragm in both anterior-superior and left-right orientation, and the radius of the curvature at the point of maximum excursion. A within-subject ANOVA was used for statistical analysis.
RESULTS
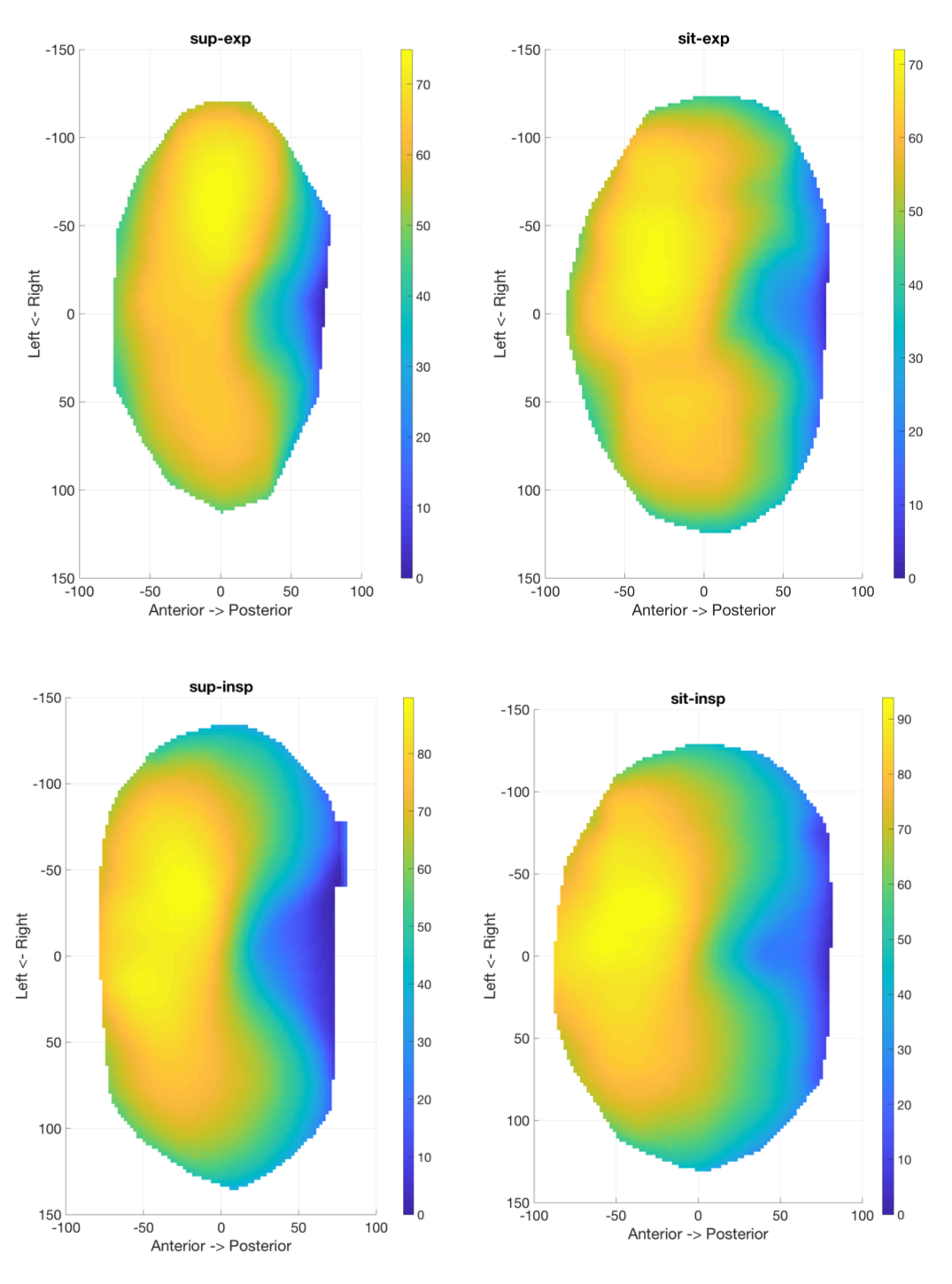
Figure 3 shows contour plots of the mean surfaces from a typical healthy subject for supine and seated position at maximum expiration (top row) and maximum inspiration (bottom row). A larger maximum excursion is noticeable at inspiration compared to expiration in both seated and supine position. The diaphragm expands laterally and the location of maximum excursion moves medially at full inspiration. The excursion at expiration is larger in seated compared to supine position.
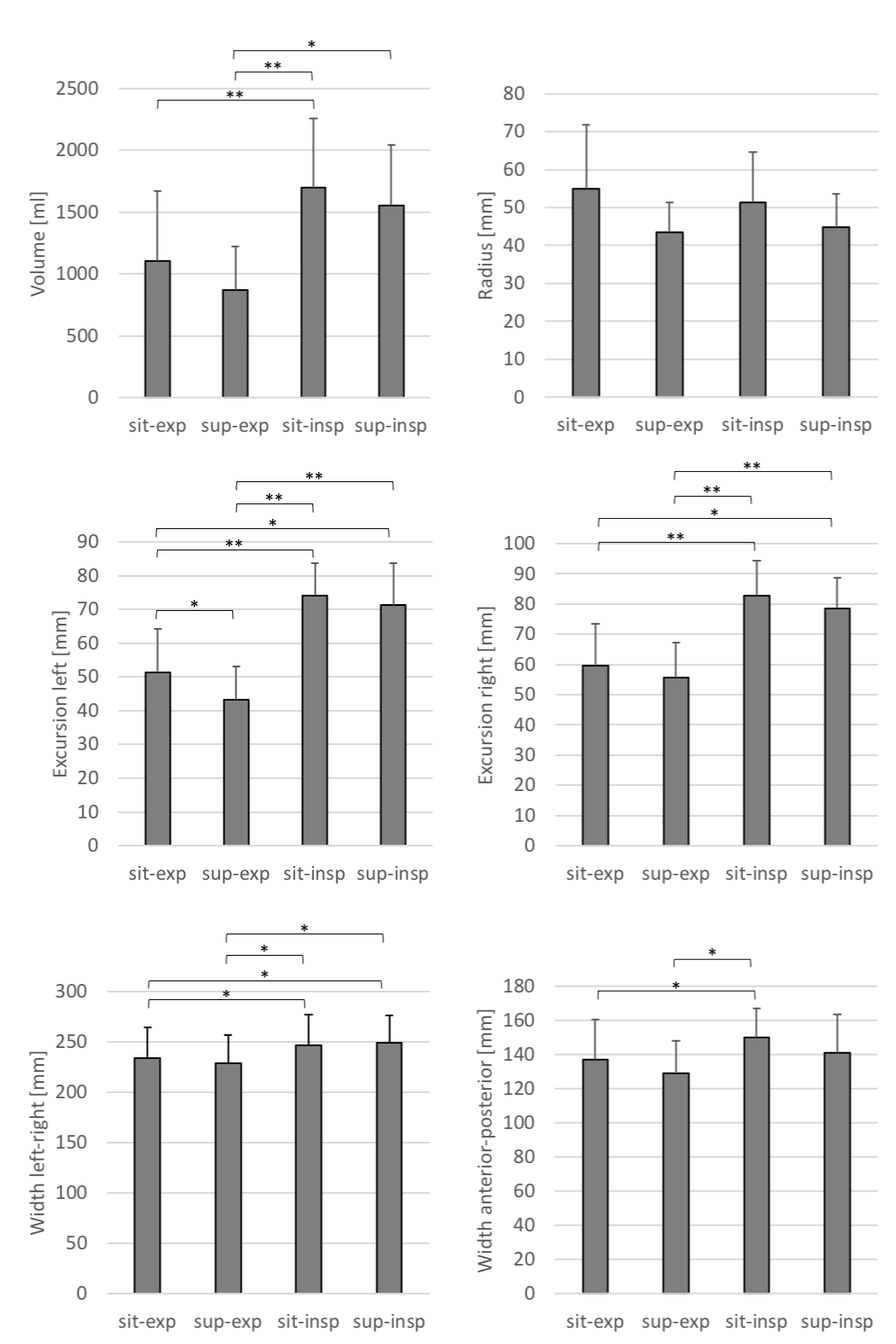
The quantitative comparison of all subjects (Fig. 4) confirmed significantly larger volume (p<.001), right and left excursion (p<.001), and right-left and anterior-posterior width (p<.05) for seated inspiration compared to seated expiration.Similarly, we found a significantly larger volume (p<.05), right and left excursion (p<.001), and right-left width (p<.05) for supine inspiration compared to supine expiration.Seated expiration showed significantly larger left excursion (p<.05) compared to supine expiration and supine inspiration had larger (p<.05) right and left excursion, and left-right width compared to seated expiration.
The breath hold duration during each scan could be reduced from initially 20 to approximately 10 seconds with our protocol.
DISCUSSION
In this pilot study we acquired scans of the diaphragm in supine and seated position at maximum inspiration and expiration with a low-field upright MR scanner. We developed a patient acceptable scanning protocol and tools for characterizing changes in diaphragm morphology. We evaluated our methods on data from healthy subjects and found significant differences in volume, excursion and width between inspiration and expiration in both supine and seated position as would be expected. We also found significant differences in excursion between seated and supine position at maximum expiration, which can be explained by the pressure on the diaphragm in supine position.
Note how the excursion and volume under the dome is larger at full inspiration. As the diaphragm contracts, the fibres attached to the Xiphisternum move cranially while the costal attachments move caudally leading to larger volume and excursion.
In the future we will apply our methods to different populations of respiratory disease patients.
CONCLUSION
The impact of posture and breath hold state on diaphragm morphology can be characterized with our novel scan protocol and analysis tools.Acknowledgements
Partly funded by the NIHR Nottingham Biomedical Research CentreReferences
1. Besl PJ, McKay ND. A Method for Registration of 3-D Shapes. IEEE Transactions on Pattern Analysis and Machine Intelligence 1992:14(2)Figures