1898
5-minute non-sedated neonatal and pediatric pulmonary UTE based MRI studies1Radiology, University of California San Francisco, San Francisco, CA, United States, 2Department of Medical Physics, University of Wisconsin, Madison, Madison, WI, United States, 3Department of Radiology, Stanford University, Stanford, CA, United States, 4Department of Electrical Engineering and Computer Sciences, UC Berkeley, Berkeley, CA, United States
Synopsis
Pulmonary MRI is free of ionizing radiation, which is beneficial for screening and longitudinal imaging in radio-sensitive populations, like newborns and children. However, practical considerations make pediatric pulmonary MRI challenging, including smaller body size, increased respiration rate, and increased motion from inability to hold still. In this work, we propose an optimized 5-minute non-sedated neonatal and pediatric pulmonary UTE, applied on seven patients.
Introduction
Computed tomography (CT) is the standard and widely used imaging technique for assessing lung anatomy, due to short scan times and high spatial resolution. But CT inevitably induces radiation exposure to patients, which is particularly concerning for neonatal and pediatric patients1. MRI would be an alternative choice for neonatal and pediatric pulmonary screening, and its flexibility also lends itself to further tissue characterization and testing of cardiac function. However, lots of challenges make neonatal and pediatric pulmonary MRI difficult. First of all, low proton density and short T2* properties largely reduce the parenchymal signal2. In addition, compared to CT, MRI requires a much longer scan time, which makes pulmonary MRI vulnerable to subject motion artifacts, especially from respiratory motion3,4. Recently, ultrashort echo time(UTE) acquisition schemes combined with motion correction strategies have been applied to pulmonary imaging in adults5,6. UTE overcomes the fast signal decay in lung parenchyma and motion correction allows free breathing scans.As for neonatal and pediatric pulmonary MRI, it is more challenging, especially for non-sedated free breathing scans. Unlike adults, it is difficult for children to keep still during a long scan and their respiration rates tend to be higher and less regular. Therefore, a limited scan time and motion robust imaging techniques are required. Additionally, most MRI hardware and software are designed with adult anatomy and physiology in mind, so these factors should also be optimized to suite the unique anatomy and physiology of children1.In this work, we propose a 5-minute non-sedated pulmonary MRI strategy based on some practical considerations in neonatal/pediatric MRI. We compare the differences between adults and pediatric studies from technical aspects, then present cases with age range from several week-old newborns to teenagers, and qualitatively compare MR scans with other product sequences, and standard clinical CT scans.Methods
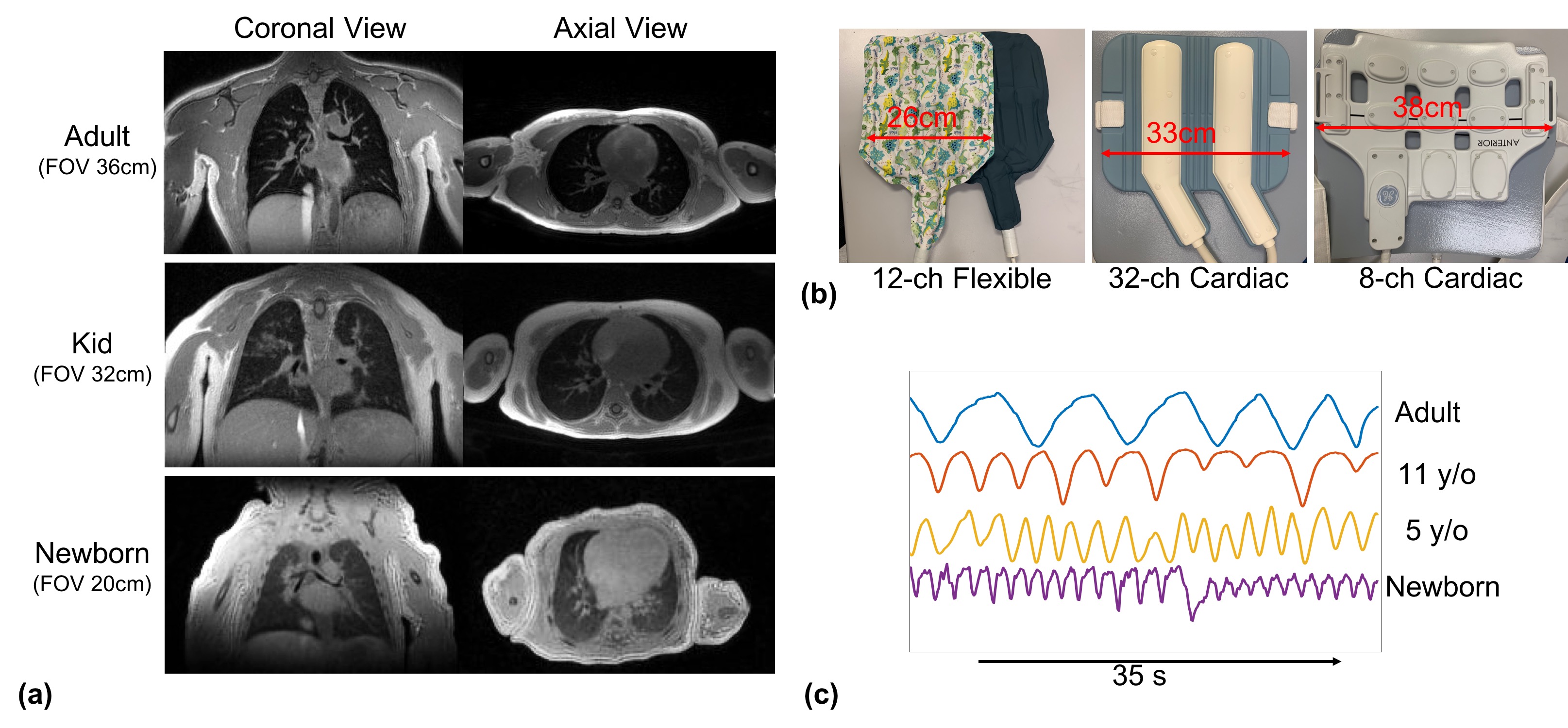
Adult and neonatal/pediatric scan comparison
A few differences between adults and pediatric scans are summarized in Figure1. Compared to adults, pediatric and neonatal studies require higher resolution for smaller lung structures, in Figure1(a), optimized receiver coils, in Figure1(b), and different motion processing strategies due to higher respiratory rate and different breathing patterns, Figure1(c).
Patient recruitment
Pediatric and neonatal patients were recruited for MRI, with Institutional Review Board approval and parental informed consent.
Acquisition, Motion Correction and Reconstruction
All the studies were run on clinical 3.0 T scanners (MR750, GE Healthcare, Waukesha, WI), having patients free breathing and without sedation. 3D 5min UTE sequence7 with golden angle ordering, and variable density readout acquisition was used for all the scans. A Self-navigator strategy was applied for tracking respiratory motion. Data with large drift in the self-navigator signal, induced by bulk motion, was removed. Then, a soft-gated reconstruction method4,8 was used for 3D high SNR motion corrected exhale state image.
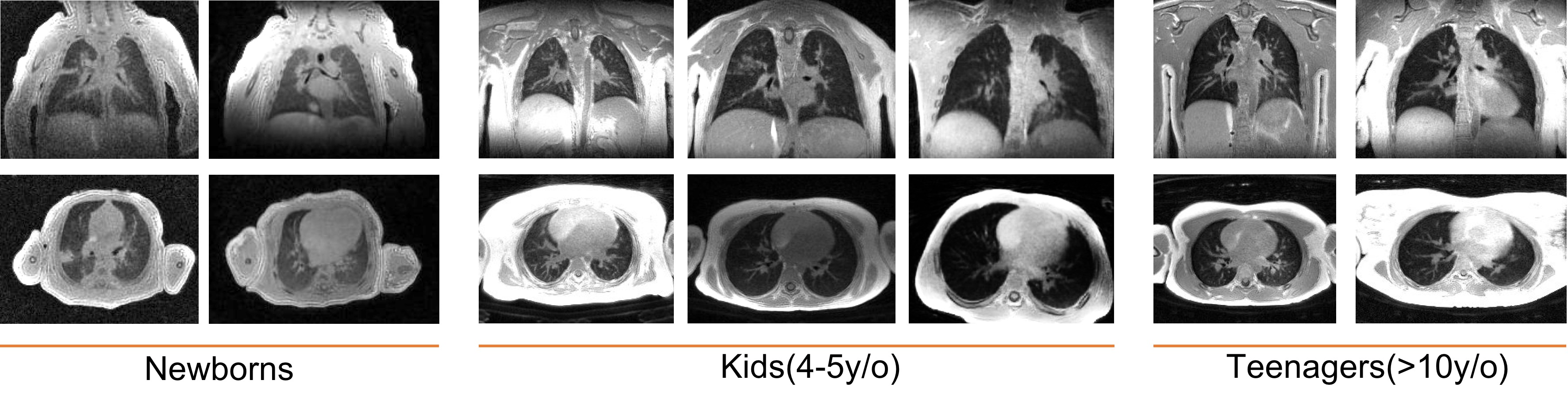
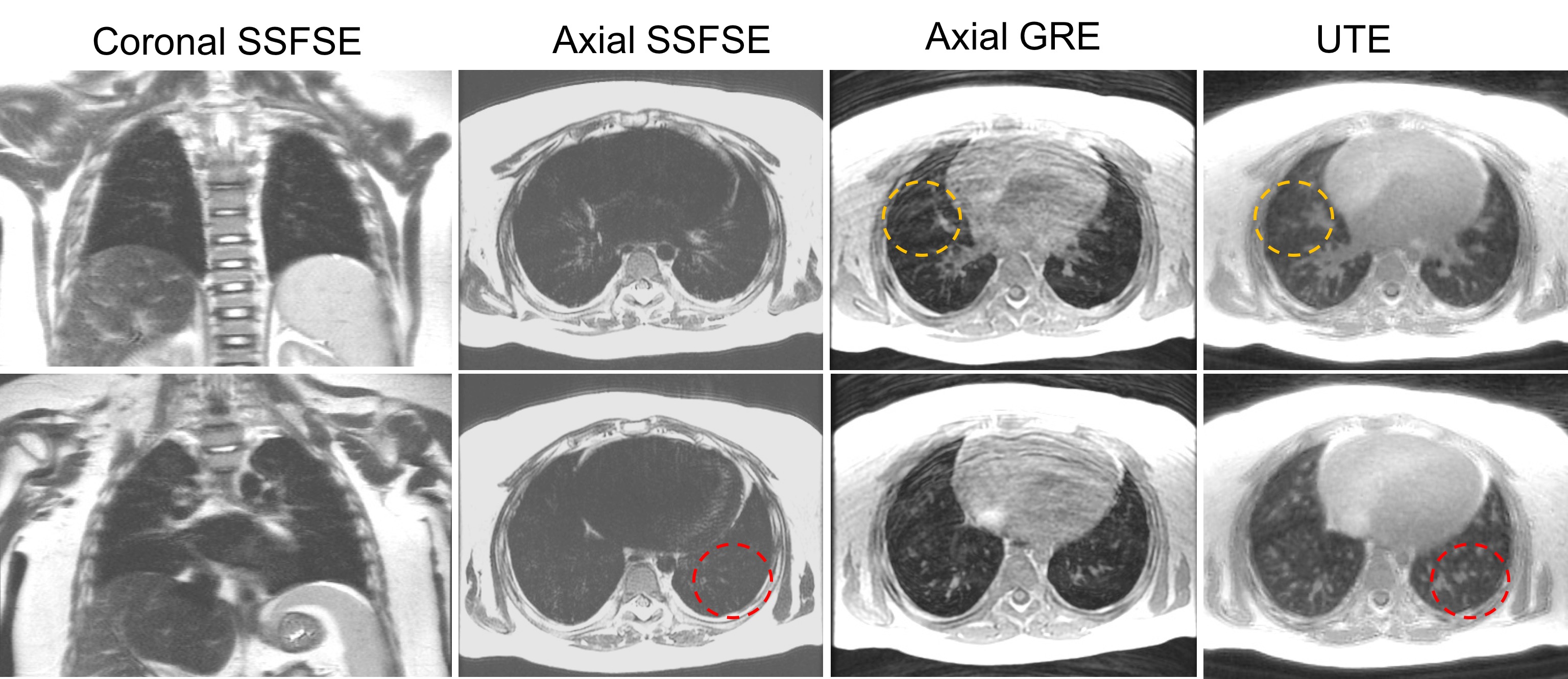
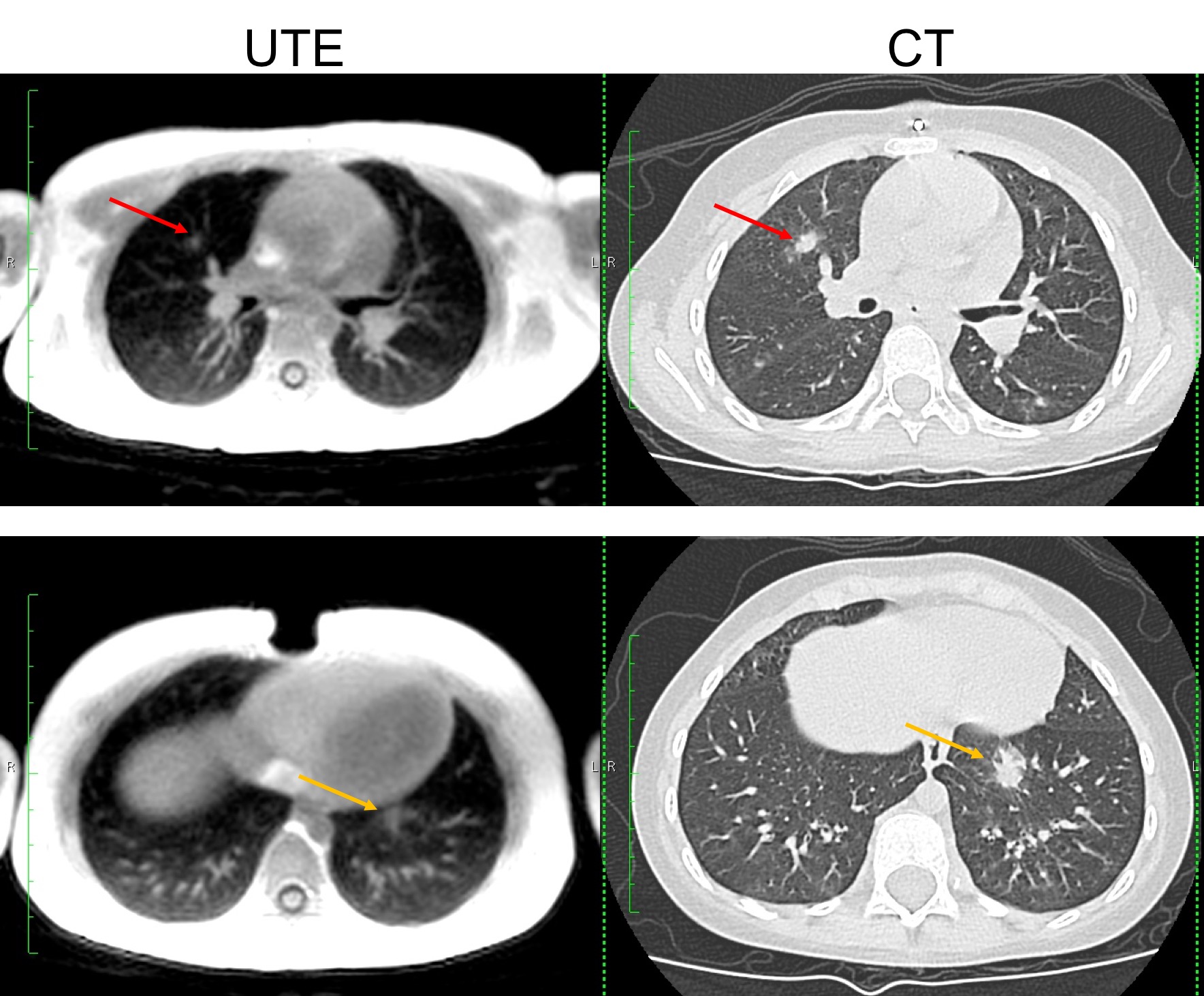
Results
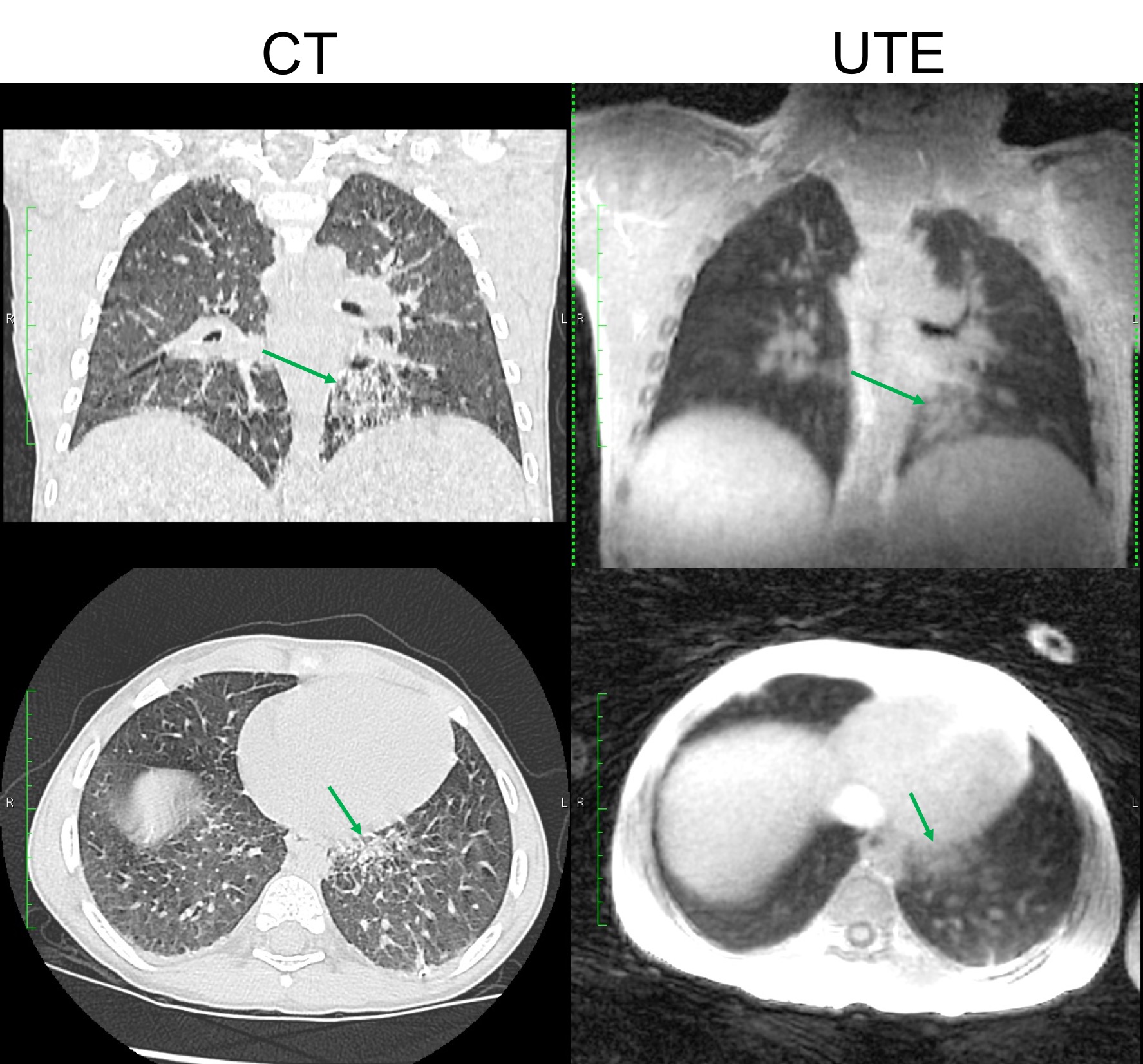
5-min free breathing UTE scans from seven subjects, including two newborns (< 1 month old), one 4-year-old and two 5 year-old kids, and two teenagers, are shown in Figure2. With optimized sequence, parameter selection, and motion correction, the images show high SNR and clear small structures (vessels and airways) in the lung.For Subject3, other sequences are acquired for comparison, summarized in Figure3. For SSFSE sequences, prospective respiratory gating with pencil-beam navigator sequence was used. Although GRE and SSFSE shows higher in plane small vessels, UTE had higher SNR, and was robust to respiratory motion, especially compared to GRE images.We also compare UTE images to standard clinical CT images on two pediatric patients. Figure 4 shows both UTE and chest CT images in an unsedated 5 year old female, where small pulmonary nodules could be distinguished from UTE images(red and orange arrows), comparable to CT scans. Figure 5 shows scans from an unsedated 4 year old male with systemic juvenile idiopathic arthritis who has childhood interstitial lung disease. He had sub pleural nodules, and ground-glass opacity observed on the CT was clearly visualized in UTE MRI(Green arrows).Conclusion
In this work, we discuss the practical considerations in neonatal and pediatric pulmonary MRI studies. Compared to adult scanning, imaging parameters, hardware setups, and motion correction need to be optimized. Our proposed 5-min free breathing non-sedated neonatal and pediatric lung UTE are highlighted, and applied to patients varied from newborns to teenagers. This approach was successful even with unsedated 4 and 5 year olds who often have trouble staying still during scans. The UTE images have high SNR and resolution in lung showing potential for a broad range of clinical applications in pediatrics and neonatology.Acknowledgements
This work is supported by NIH grant R01 HL136965.References
1. Hahn AD, Higano NS, Walkup LL, et al. Pulmonary MRI of Neonates in the Intensive Care Unit Using 3D Ultrashort Echo Time and a Small Footprint MRI System. J Magn Reson Imaging. 2016;45(2):463-471. doi:10.1002/jmri.25394.
2. Yu J, Xue Y, Song HK. Comparison of lung T2* during free-breathing at 1.5 T and 3.0 T with ultrashort echo time imaging. Magn Reson Med. 2011;66(1):248-254. doi:10.1002/mrm.22829.
3. Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med. 2015;00(October 2014):n/a-n/a. doi:10.1002/mrm.25665.
4. Cheng JY, Zhang T, Ruangwattanapaisarn N, et al. Free-breathing pediatric MRI with nonrigid motion correction and acceleration. J Magn Reson Imaging. 2015;42(2):407-420. doi:10.1002/jmri.24785.
5. Feng L, Delacoste J, Smith D, et al. Simultaneous Evaluation of Lung Anatomy and Ventilation Using 4D Respiratory- Motion-Resolved Ultrashort Echo Time Sparse MRI. 2018:1-12. doi:10.1002/jmri.26245.
6. Jiang W, Ong F, Johnson KM, et al. Motion Robust High Resolution 3D Free-Breathing Pulmonary MRI Using Dynamic 3D Image Self-Navigator. 2018;2967(October 2017):2954-2967. doi:10.1002/mrm.26958.
7. Johnson KM, Fain SB, Schiebler ML, Nagle S. Optimized 3D ultrashort echo time pulmonary MRI. Magn Reson Med. 2013;70(5):1241-1250. doi:10.1002/mrm.24570.
8. Johnson KM, Block WF, Reeder SB, Samsonov A. Improved Least Squares MR Image Reconstruction Using Estimates of k- Space Data Consistency. 2012;1608:1600-1608. doi:10.1002/mrm.23144.
Figures