1897
Compressed Sensing reconstruction in non-contrast-enhanced functional lung MRI using Fourier Decomposition: An initial study1Computer Assisted Clinical Medicine, Heidelberg University, Mannheim, Germany
Synopsis
Ventilation and perfusion functions have significant clinical value for the diagnosis of pulmonary diseases. Fourier Decomposition is a non-contrast-enhanced method for assessing regional ventilation and perfusion information from time-resolved images. However, its robustness suffers from poor temporal resolution. Here we propose a compressed sensing reconstruction of undersampled acquisitions to improve temporal resolution of dynamic images. Retrospective demonstrations on in vivo acquisitions indicate that the proposed reconstruction scheme achieves similar image quality to conventional acquisitions while improving scan efficiency.
Introduction
Assessment of local pulmonary ventilation and perfusion has significant clinical value for the diagnosis and follow-up of lung diseases. Although the gold standard for functional lung assessment depends on methods using radioactive nuclides, non-ionizing methods are highly desirable1. In an earlier study, Fourier Decomposition was demonstrated to be a useful non-contrast-enhanced MRI method to assess perfusion and ventilation1. By utilizing a 2D fast imaging sequence, a set of dynamic images during free breathing is acquired and registered to a reference image. Afterwards, images are analyzed voxel-wise using Fourier transform to obtain periodic signal variations corresponding to respiratory and cardiac signal modulations. Subsequently, ventilation-weighted and perfusion-weighted images are generated.
While numerous studies have validated the FD method against well-established methods, its robustness critically depends on temporal resolution2. Here, we propose an approach based on random undersampling in the phase encoding dimension with regularized reconstruction to improve the acquisition time and consequently, the temporal resolution of image series. In vivo results are presented to demonstrate the performance of proposed method.
Methods
2D balanced steady-state free precession images were acquired of a healthy volunteer (female, 29 years old) during free-breathing using a 1.5 T scanner (Magnetom Avanto, Siemens Healthineers, Erlangen, Germany) with the following parameters: TR/TE = 1.88/0.80 ms, slice thickness 15 mm, FOV = 450 mm X 450 mm, matrix size = 128 X 128, GRAPPA factor = 2, bandwidth = 1302 Hz/Px, flip angle = 50°. A total of 210 images were acquired with a 0.1 s pause after each measurement. Total scan time was 49 seconds. To shorten the echo time, asymmetric echo was allowed1. The acquisitions were then registered using a stand-alone non-rigid registration software3.
The dataset was retrospectively undersampled in the phase encoding dimension to yield acceleration factors (R) of 2-6, using variable density random sampling4. Different sampling patterns were generated to extent k-space coverage across measurements5. The reconstructions were obtained by solving the following optimization problem:
$$ \min\parallel F_p \cdot m-y\parallel+\lambda \parallel T \cdot m\parallel_1$$
Here, $$$F_p$$$ is the Partial Fourier operator, $$$m$$$ is the reconstruction, $$$y$$$ is the acquired k-space data, $$$\lambda$$$ is the sparsity penalty weight, and $$$T$$$ represents the sparsifying transform. In this work, we have used temporal total variation as the sparsifying transform to exploit temporal correlations and sparsity in the dynamic data6. The penalty weight was empirically selected and was fixed as $$$\lambda=0.39$$$ for all acceleration rates.
To quantitatively compare the reconstructions, structural similarity index metric (SSIM)7 and ratio metrics were utilized. Ratio metric was defined as pixel-wise division of the normalized reconstruction to normalized reference image. Both metrics were calculated with respect to the fully sampled reference data (R=1), over a cropped rectangular field of view covering the lung parenchyma to better reflect the reconstruction performance.
Results
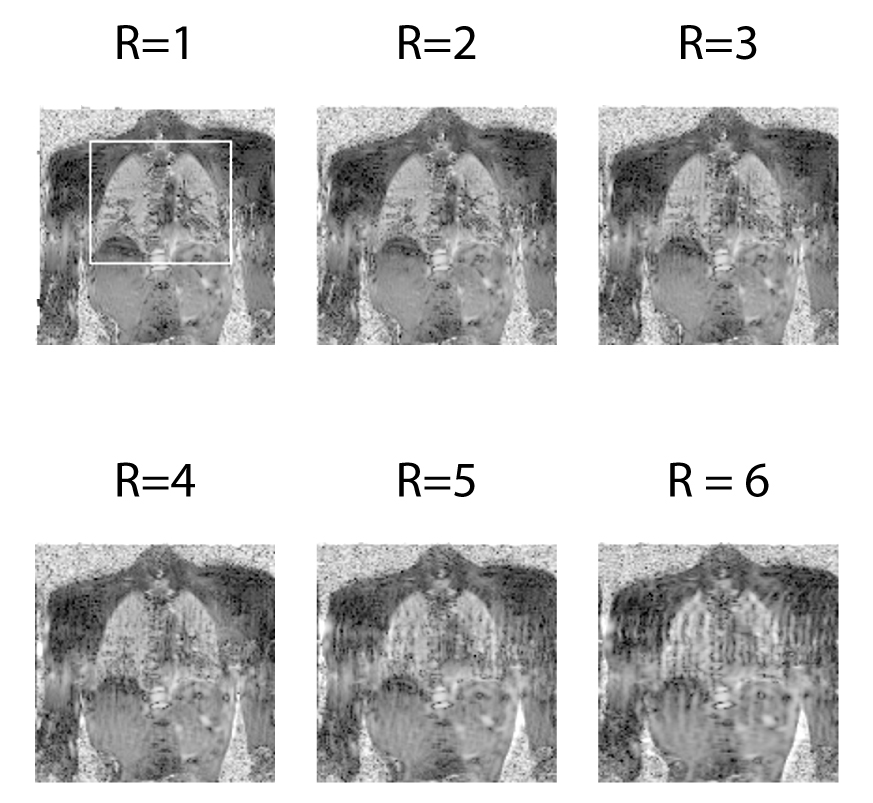
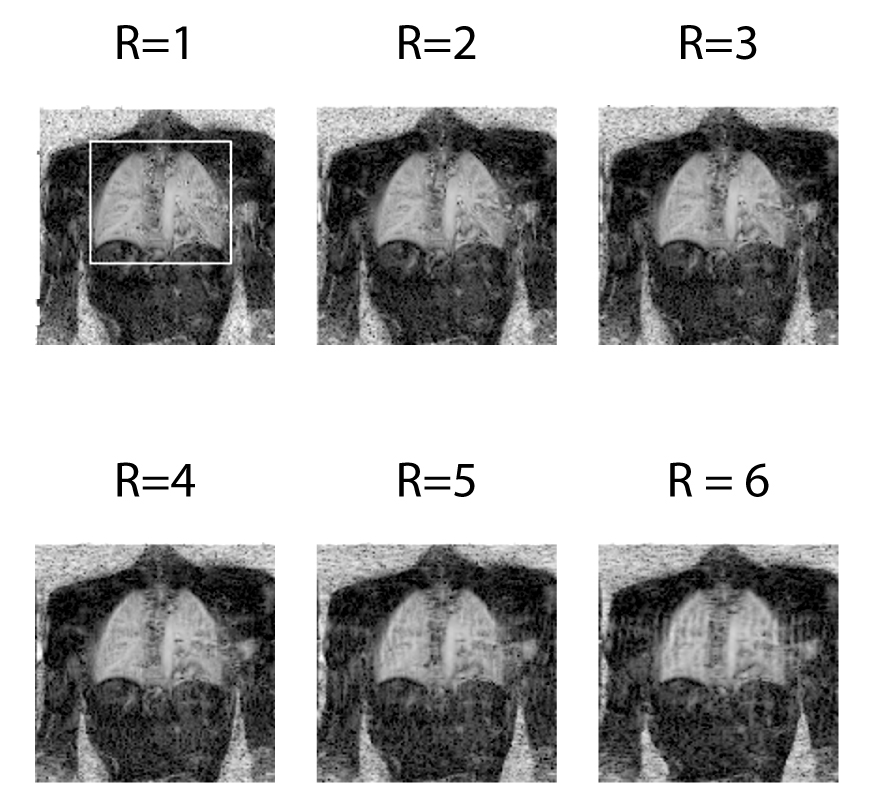
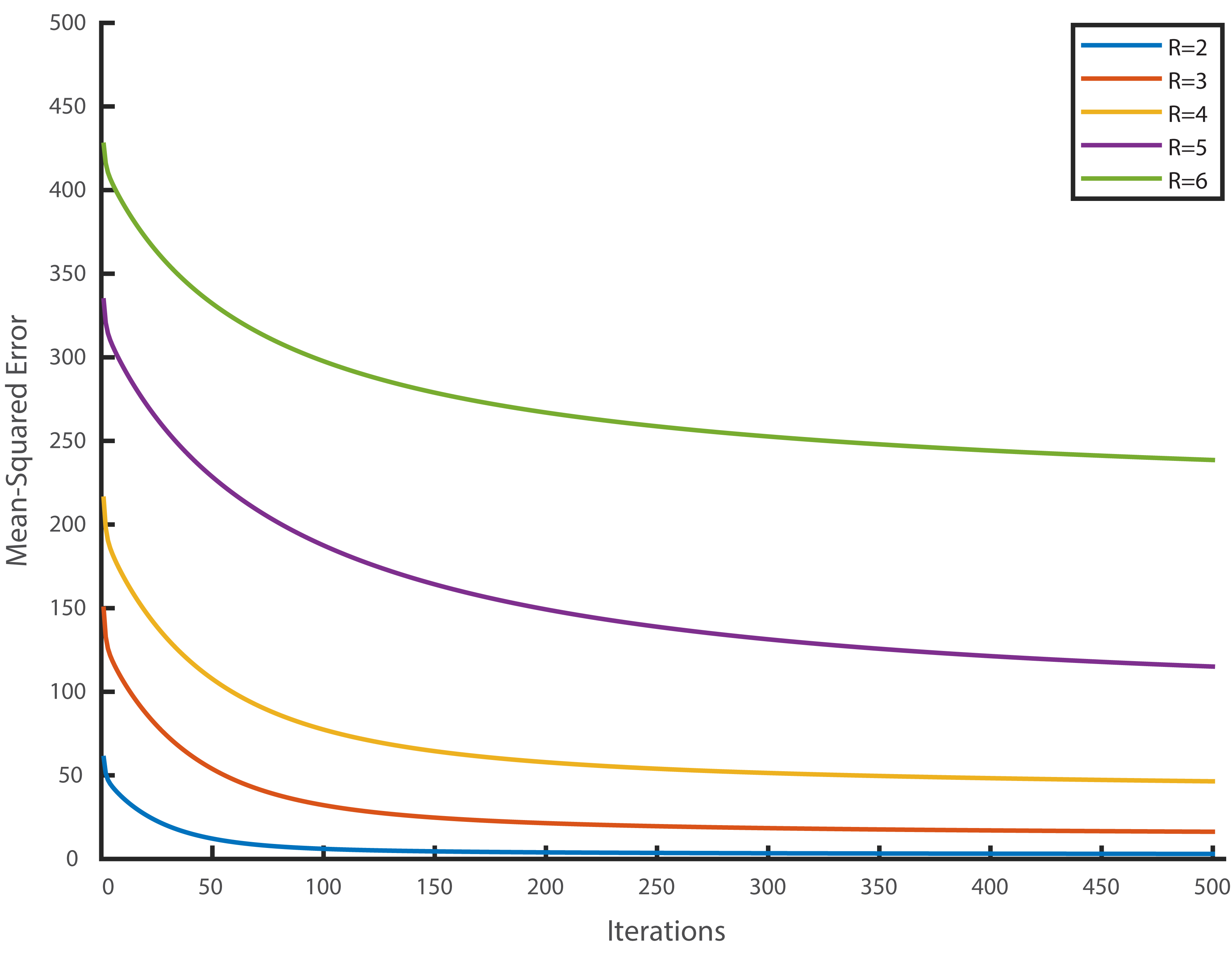
Figure 1 and 2 show the ventilation and perfusion weighted images. For ventilation and perfusion weighted images, the proposed method is able to achieve similar image quality compared to fully sampled acquisitions up to R=4 and R=5, respectively. These observations are reflected in SSIM and ratio metric values as noted in Table 1. For R>5, the SSIM values drop below 0.6 due to interference, meanwhile the ratio values remain close to 1; suggesting degradation in image quality without a significant deviation from actual ventilation and perfusion values. Figure 3 shows the convergence behavior of our method for different acceleration rates. As expected, higher acceleration rates produce higher mean-squared error, and with fixed penalty weight, reconstructions required higher number of iterations before converging. Overall, our results indicate that compressed sensing can be utilized to decrease the acquisition time to improve temporal resolution in functional lung imaging.Discussion and Conclusion
In this work, we have used retrospectively undersampled dynamic lung acquisitions to evaluate the usefulness of compressed sensing with the Fourier Decomposition method. Although future studies with more subjects and with prospective undersampling are warranted, our preliminary results indicate that improved scan efficiency or higher temporal resolutions can be achieved via compressed sensing reconstructions. In vivo results demonstrate that the proposed method is able to achieve images of equivalent quality to reference images. These observations were supported by quantitative measurements.
To our knowledge, this work represents the first investigation of the Fourier Decomposition method with a compressed sensing reconstruction. Our results indicate that the proposed method can to improve temporal resolution of free breathing non-contrast-enhanced functional lung MRI studies, and promises increased clinical value for the diagnosis and follow-up of pulmonary diseases.
Acknowledgements
This work was supported by Deutsche Forschungsgemeinschaft (grant number: DFG 397806429).References
1. Bauman, G. , Puderbach, M. , Deimling, M. et al. Non‐contrast‐enhanced perfusion and ventilation assessment of the human lung by means of Fourier decomposition in proton MRI. Magn. Reson. Med. 2009;62:656-664.
2. Kjørstad A, Corteville DM, Henzler T, et al. Quantitative lung ventilation using Fourier decomposition MRI: comparison and initial study. MAGMA 2014;27(6):467–476.
3. Chefd’hotel C, Hermosillo G, Faugeras O. Flows of diffeomorphisms for multimodal image registration. Proceedings IEEE International Symposium on Biomedical Imaging. 2002;753–756.
4. Lustig, M. , Donoho, D., Pauly, J. M. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magn. Reson. Med. 2007;58:1182-1195.
5. Ilicak, E. , Senel, L. K., Biyik, E., et al. Profile‐encoding reconstruction for multiple‐acquisition balanced steady‐state free precession imaging. Magn. Reson. Med. 2017;78:1316-1329.
6. Feng, L. , Grimm, R. , Block, K. T, et al. Golden‐angle radial sparse parallel MRI: Combination of compressed sensing, parallel imaging, and golden‐angle radial sampling for fast and flexible dynamic volumetric MRI. Magn. Reson. Med. 2014;72:707-717.
7. Qing, K. , Altes, T. A., Tustison, N. J., et al. Rapid acquisition of helium‐3 and proton three‐dimensional image sets of the human lung in a single breath‐hold using compressed sensing. Magn. Reson. Med. 2015;74:1110-1115.
Figures