1885
Ventilation Defect Percent from Hyperpolarized Helium-3 MRI as a predictor of Asthma Exacerbation Severity1Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 2Biomedical Engineering, University of Wisconsin-Madison, Madison, WI, United States, 3Biostatistics and Medical Informatics, University of Wisconsin-Madison, Madison, WI, United States, 4Pulmonary and Critical Care Medicine, University of Kansas Medical Center, Kansas City, KS, United States, 5Radiology, University of Wisconsin-Madison, Madison, WI, United States, 6Pharmacy, University of Wisconsin-Madison, Madison, WI, United States, 7Radiology, Washington University St. Louis, St. Louis, MO, United States, 8Center for Pulmonary Imaging Research, University of Cincinnati Children's Hospital, Cincinnati, OH, United States, 9Allergy, Pulmonary, & Critical Care Medicine, University of Wisconsin-Madison, Madison, WI, United States, 10Pulmonary and Critical Care Medicine, Washington University St. Louis, St. Louis, MO, United States
Synopsis
We assessed ventilation defect percent (VDP) on hyperpolarized (HP) 3He MRI in 28 asthmatics at baseline and recovery visits following an exacerbation (10 ± 7 months apart). We found that pre-bronchodilator VDP at baseline was a stronger predictor of severe exacerbations than conventional asthma control indices, and subjects that underwent a severe exacerbation had highly variable VDP changes after recovery. These findings suggest that VDP is a potential biomarker of asthma instability.
Introduction
Ventilation defects on hyperpolarized gas magnetic resonance imaging (HP gas MRI) can be characterized using the ventilation defect percent (VDP). VDP has previously been associated retrospectively with severe clinical outcomes in asthma1 and has also been shown to be predictive of any exacerbation within the following year2. We hypothesize that VDP measured on HP gas MRI may be predictive of exacerbation severity in asthma subjects.Methods
Participants from 2 sites of the longitudinal Severe Asthma Research Program (SARP3) underwent baseline (BL) HP 3He MRI and were recruited for subsequent evaluation scheduled at the onset of acute upper respiratory symptoms, some of whom also had a severe exacerbation, defined as the need of 3 or more days of oral corticosteroids (OCS). Spirometry and imaging were performed before and after administration of four puffs of albuterol (“pre-BD” and “post-BD” respectively). Characterization at the acute visit included symptom surveys, medication use updates, and lung function measurements. Imaging was also performed at least 6 weeks after the participants recovered, termed the post respiratory symptoms (PRS) visit. The defect burden was measured using the whole lung VDP for both study visits, as previously described3.We used a Wilcoxon rank-sum test to compare measurements, logistic regression and ROC analysis to compare predictors of exacerbation, Levene’s variance test to compare the distribution of VDP difference between visits (∆VDP), and Spearman’s correlation to compare changes in VDP.Results
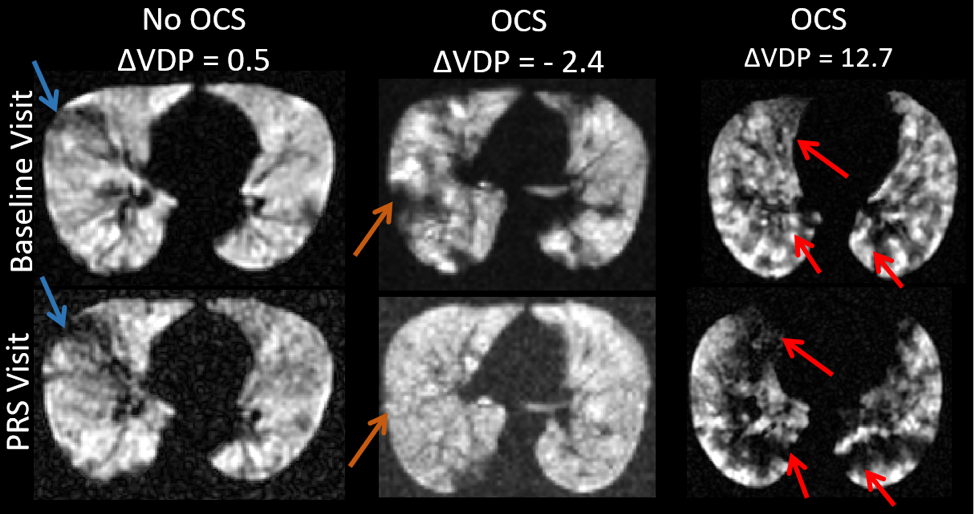
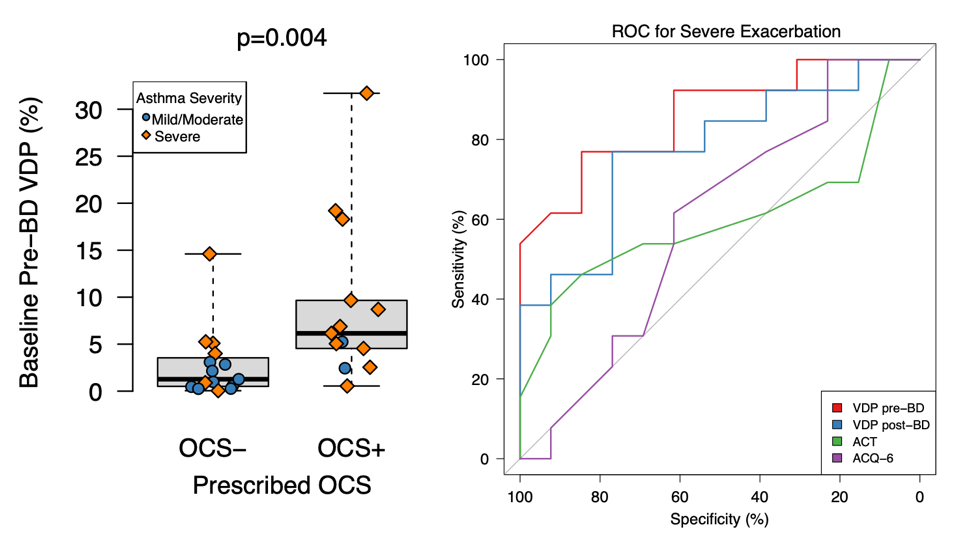
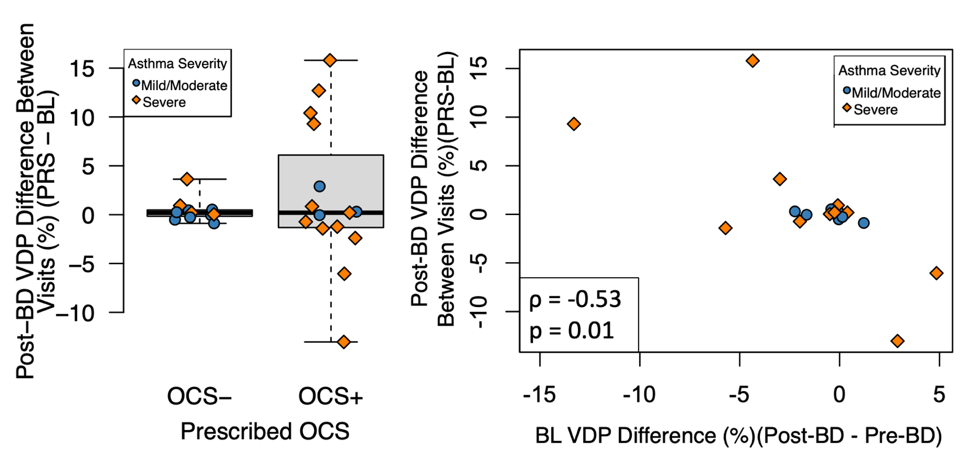
Twenty-eight participants (11 mild-to-moderate and 17 severe asthmatics) had complete data including imaging at both the baseline and recovery visits. 15 participants had a severe exacerbation. Exemplary results from subjects with a range of VDP and exacerbation outcomes are shown in Figure 1. Participants with a severe exacerbation had significantly higher baseline pre-BD VDPs than participants who did not (p = 0.004), Figure 2. BL pre-BD VDP was found to be the strongest predictor of exacerbation (AUC=86.1% with a threshold of 4% VDP) when compared to the asthma control test (ACT), the asthma control questionnaire (ACQ), spirometry measures (pre- and post-BD FEV1 and FVC percent predicted), and post-BD VDP. Disease severity (mild-to-moderate or severe) plus BL pre-BD VDP was a better predictor of severe exacerbation than disease severity alone (p=0.04). Participants with a severe exacerbation had a more variable ∆VDP between recovery and baseline visits (p = 0.01), Figure 3. The ∆VDP between the recovery and baseline visits was found to be negatively associated with the BL bronchodilator response ∆VDP (ρ= -0.53, p = 0.01).Discussion
Whole lung pre-BD VDP on HP 3He MRI is a strong prospective predictor of severe exacerbations in asthma. The response of VDP to OCS treatment was inconsistent between asthmatics, but subjects with higher VDP reversibility after bronchodilator at the baseline visit (e.g. had a lowered Post-BD VDP) had greater VDP at the PRS visit suggesting greater instability of airway obstruction.Conclusions
Prospectively measured pre-BD VDP from HP 3He MRI is predictive of asthma exacerbation severity. Participants that underwent a severe exacerbation have more unpredictable changes in their VDP after recovery and these changes were negatively associated with bronchodilator response at baseline. Identifying VDP pre-/post-bronchodilator response may therefore be useful to predict longitudinal extent and stability of asthma.Acknowledgements
The authors would like to acknowledge funding from RO1 HL115118 and U10 HL109168, as well as funding from GE Healthcare for MRI research at UW-Madison.References
1. D. G. Mummy et al., “Ventilation defect percent in helium-3 magnetic resonance imaging as a biomarker of severe outcomes in asthma,” J. Allergy Clin. Immunol., vol. 141, no. 3, pp. 1140-1141. e4, 2018.
2. D. Mummy, “High Ventilation Percent on Hyperpolarized Helium-3 MRI is Associated with Reduced One-Year Risk of Asthma Exacerbation,” ISMRM 2018, vol. Abstract 4463.
3. W. Zha et al., “Regional Heterogeneity of Lobar Ventilation in Asthma Using Hyperpolarized Helium-3 MRI,” Acad. Radiol., 2017.
Figures