1876
A new approach to quantitative measurement of breast tumor blood flow, capillary permeability, and interstitial pressure.1Radiology, University of Chicago, Chicago, IL, United States, 2Statistics, University of Chicago, Chicago, IL, United States, 3Biomedical Engineering, University of Texas at Austin, Austin, TX, United States, 4Institute for Computational and Engineering Sciences, Diagnostic Medicine, and Oncology, University of Texas at Austin, Austin, TX, United States
Synopsis
Ultrafast DCE-MRI detects sparse enhancement during the early phase of contrast media uptake [8]. This facilitates reconstruction of arteries and lesions using partial k-space data to obtain even higher temporal resolution. In addition, new approaches to tracking blood vessels in breast [10] identify arteries feeding suspicious lesions and possibly also draining veins. As a result, tumor blood flow can be accurately measured from propagation of the contrast media bolus along arteries that supply tumors. This approach avoids assumptions and artifacts that are inherent in pharmacokinetic analysis, and facilitates measurement of important biomarkers, e.g. capillary permeability and interstitial pressure.
INTRODUCTION
Measurements of tumor blood flow based on pharmacokinetic analysis of contrast media kinetics depends on compartmental models for tissue [1, 2]. These models do not match the true breast tissue structure [3, 4], and this can cause significant errors in data analysis. Here we identify arteries feeding the lesion, track the speed of propagation of the bolus down each artery, and measure arterial diameter to measure blood flow to the tumor. We use ultrafast data acquisition [3, 5-8] and partial k-space reconstruction to obtain bilateral images of enhancing arteries and lesions with high temporal resolution. This method, combined with pharmacokinetic measurements [9] of Ktrans (volume transfer coefficient) may allow measurement of tumor permeability. In addition, tumor interstitial pressure can be evaluated from the speed of bolus propagation [10, 11]. These are two important biomarkers that cannot be measured by conventional pharmacokinetic measurements alone. This method was tested using simulations based on breast models constructed from actual ultrafast DCE-MRI (dynamic contrast enhanced MRI) data.THEORY AND METHODS
Bilateral breast images ultrafast (3.5 seconds/image) DCE images (contrast agent dose = 0.1 mM/kg) were acquired on a Philips 3T scanner. These images were used to produce a breast model that simulated the Parker AIF [12] propagating along internal mammary arteries and the single artery feeding the cancer with 50 msec resolution. A full k-space dataset was acquired every 3.5 seconds. Each ¼ second section of k-space, calculated from the 50 msec simulation, was used to estimate a bilateral image by optimizing over a regularized temporal smoothing constraint via gradient descent (analogous to [13]).RESULTS
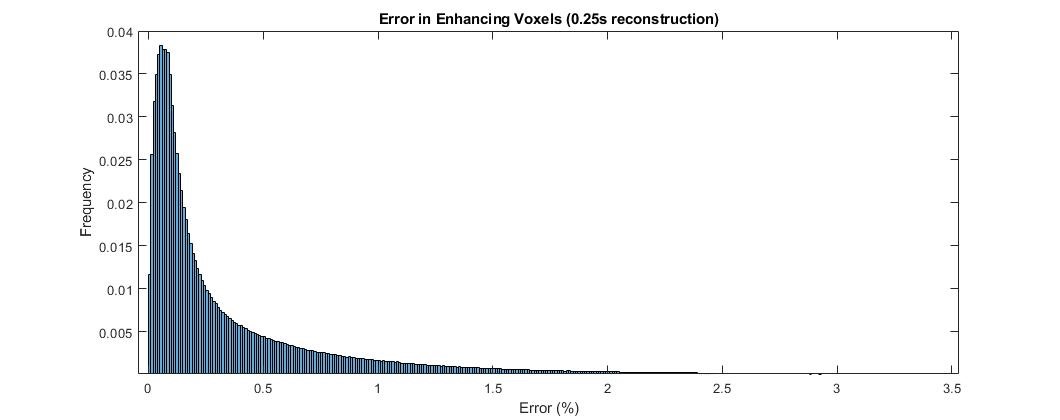
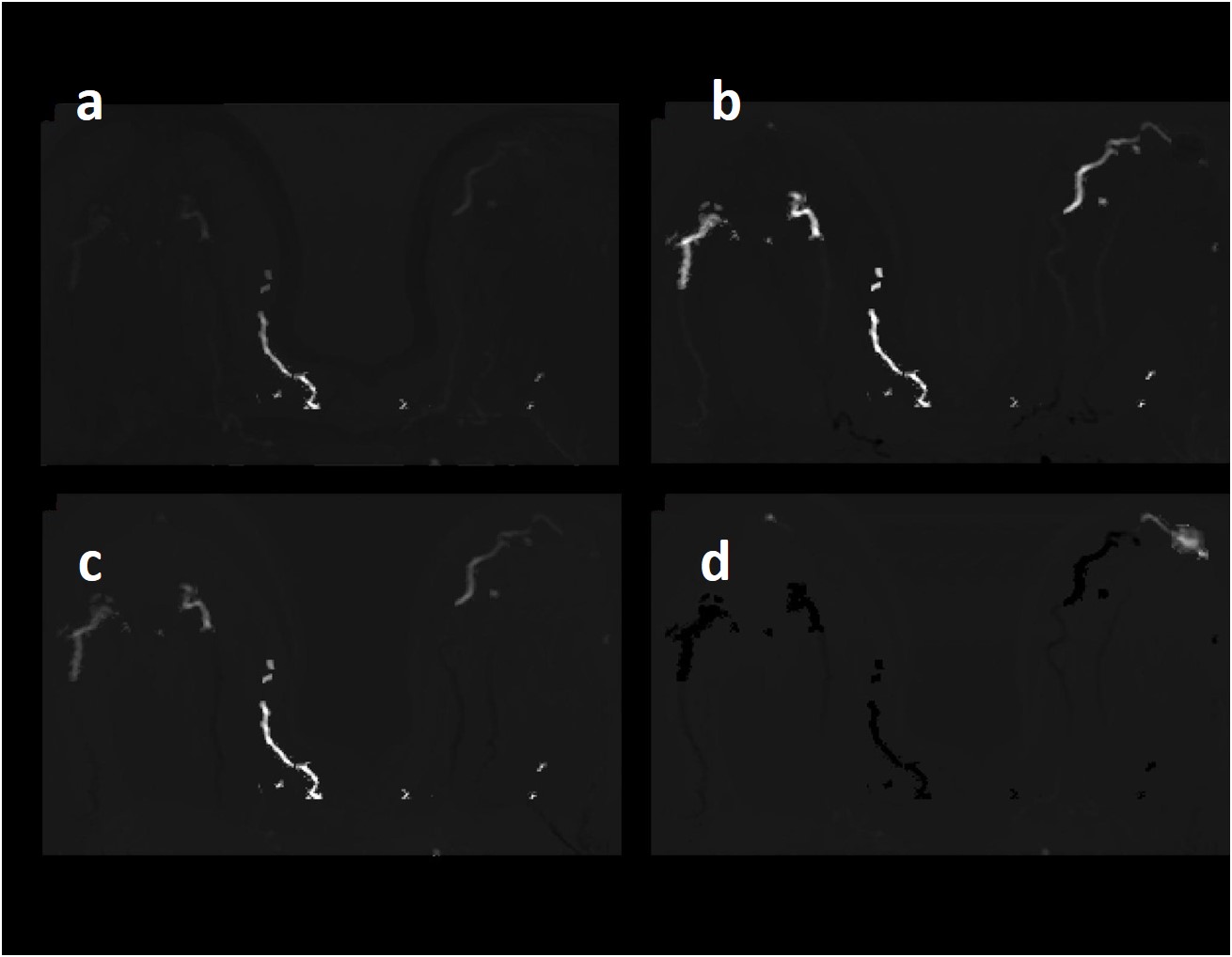
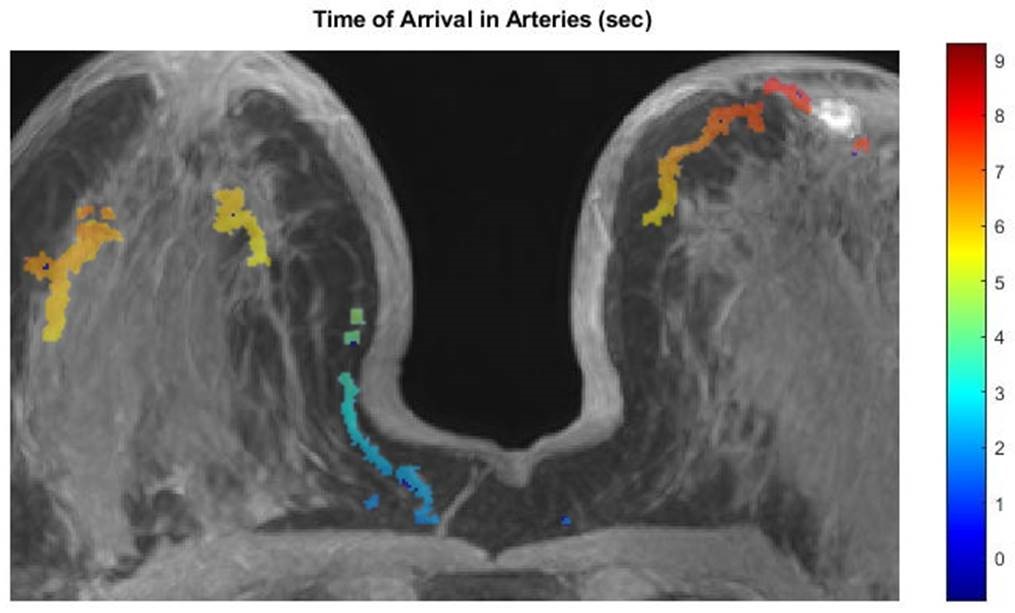
Image reconstructions using 1/14th of a complete k-space dataset closely matched the ‘gold standard’ fully sampled images simulated with 50 msec temporal resolution. 98% of enhancing voxels had error (difference between gradient descent reconstructions and ‘gold standard’ images) of 2% or less (see Figure 1). Gradient subtraction images (each image subtracted from the subsequent image) reconstructed from 1/14th of k-space (Figure 2), clearly show the single artery feeding the breast cancer, as well as other arteries and the suspicious lesion. Figure 3 shows the time of arrival of the contrast media bolus at each point along each artery (blue = early arrival; red = later arrival). Based on these measurements the speed of propagation of the AIF, i.e. the speed of blood flow, is ~2.2 cm/sec near the lesion. The diameter of the artery feeding the lesion is 1.5 mm and plasma flow (0.55 * blood flow) to the lesion is approximately 1.3 mls per minute. The volume of the lesion, based on enhancement in later post contrast images is ~1.57 grams, so lesion perfusion is ~0.83 mls of plasma per gram of tissue per minute. This is equivalent to an average lesion Ktrans of 0.83 min-1, assuming high permeability, i.e. extraction fraction of 1.0.CONCLUSION
Ultrafast DCE-MRI facilitates reconstruction of images from partial k-space data is effective because the difference images during initial enhancement are very sparse [7, 8, 14]. The gradient descent [13] method provided accurate reconstructions at ¼ sec temporal resolution (Figures 2 and 3). This was critical for accurate measurement of the speed of blood flow in arteries. Although a full contrast agent dose was used here, a much lower dose could be used for more accurate detection of the bolus [15]. The speed of blood flow and arterial lumen diameter measured from high temporal resolution images were used to determine the rate of blood flow. With real data, capillary permeability would be determined by comparing Ktrans determined from arterial blood flow to the average Ktrans from pharmacokinetic modeling. In the data shown here the single artery feeding the tumor is easily identified. In more complicated cases, the vessel tracking method developed by Wu et al [10] can identify arteries feeding breast cancers, and possibly draining veins. This approach to measurement of tumor blood flow avoids errors due to use of compartmental models [2, 9] that are not a good match for tissue microstructure [2, 16], and errors due to the assumption that all compartments are well mixed [4]. In addition, tumor interstitial pressure can be measured based on speed of blood flow in arteries feeding tumors versus arteries feeding normal tissue [11, 17]. These biomarkers are important indicators of cancer malignancy and response to therapy. Finally, this approach may allow measurement of tumor blood flow with low doses of contrast agent, since bolus propagation can be measured more accurately and with high SNR at very low contrast media concentrations [15].Acknowledgements
This research is supported by National Institutes of Health (R01 CA172801-01, R01 CA218700-01, and 5U01 CA142565-09, and U01CA174706), and the Segal Foundation.References
1. Yankeelov, T.E. and J.C. Gore, Dynamic Contrast Enhanced Magnetic Resonance Imaging in Oncology: Theory, Data Acquisition, Analysis, and Examples. Curr Med Imaging Rev, 2009. 3(2): p. 91-107.
2. Sourbron, S.P. and D.L. Buckley, Classic models for dynamic contrast-enhanced MRI. NMR Biomed, 2013. 26(8): p. 1004-27.
3. Jansen, S.A., et al., Ductal carcinoma in situ: X-ray fluorescence microscopy and dynamic contrast-enhanced MR imaging reveals gadolinium uptake within neoplastic mammary ducts in a murine model. Radiology, 2009. 253(2): p. 399-406.
4. Woodall, R.T., et al., The effects of intravoxel contrast agent diffusion on the analysis of DCE-MRI data in realistic tissue domains. Magn Reson Med, 2018. 80(1): p. 330-340.
5. Mann, R.M., et al., A novel approach to contrast-enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Invest Radiol, 2014. 49(9): p. 579-85.
6. Pinker, K., et al., A combined high temporal and high spatial resolution 3 Tesla MR imaging protocol for the assessment of breast lesions: initial results. Invest Radiol, 2009. 44(9): p. 553-8.
7. Abe, H., et al., Kinetic Analysis of Benign and Malignant Breast Lesions With Ultrafast Dynamic Contrast-Enhanced MRI: Comparison With Standard Kinetic Assessment. AJR Am J Roentgenol, 2016. 207(5): p. 1159-1166.
8. Pineda, F.D., et al., Ultrafast Bilateral DCE-MRI of the Breast with Conventional Fourier Sampling: Preliminary Evaluation of Semi-quantitative Analysis. Acad Radiol, 2016. 23(9): p. 1137-44.
9. Tofts, P.S. and A.G. Kermode, Measurement of the blood-brain barrier permeability and leakage space using dynamic MR imaging. 1. Fundamental concepts. Magn Reson Med, 1991. 17(2): p. 357-67.
10. Wu, C., et al., Quantitative analysis of vascular properties derived from ultrafast DCE-MRI to discriminate malignant and benign breast tumors. Magn Reson Med, 2018.
11. Wu C, P.F., Hormuth DA, Karczmar G, Yankeelov TE. . Computational fluid dynamics characterizing flow through breast tumors using patient-specific geometries. . in Annual meeting of BMES. 2018.
12. Parker, G.J., et al., Experimentally-derived functional form for a population-averaged high-temporal-resolution arterial input function for dynamic contrast-enhanced MRI. Magn Reson Med, 2006. 56(5): p. 993-1000.
13. Ryan Wen Liu, L.S., Simon Chun Ho Yu, Naixue Xiong,Defeng Wang, Reconstruction of Undersampled Big Dynamic MRI Data Using Non-Convex Low-Rank and Sparsity Constraints Sensors, 2017. 17(3): p. 509.
14. Jansen, S.A., et al., Characterizing early contrast uptake of ductal carcinoma in situ with high temporal resolution dynamic contrast-enhanced MRI of the breast: a pilot study. Phys Med Biol, 2010. 55(19): p. N473-85.
15. He, D., et al., Feasibility of Dynamic Contrast-Enhanced Magnetic Resonance Imaging Using Low-Dose Gadolinium: Comparative Performance With Standard Dose in Prostate Cancer Diagnosis. Invest Radiol, 2018. 53(10): p. 609-615.
16. Sourbron, S.P. and D.L. Buckley, On the scope and interpretation of the Tofts models for DCE-MRI. Magn Reson Med, 2011. 66(3): p. 735-45.
17. Liu, L.J., et al., Estimation of Tumor Interstitial Fluid Pressure (TIFP) Noninvasively. PLoS One, 2016. 11(7): p. e0140892.
Figures