1875
Preliminary study of diffusion kurtosis imaging in differential diagnosis of benign and malignant breast lesions1The Second Hospital of Dalian Medical University, Dalian, China, 2GE Healthcare, Beijing, China
Synopsis
Objective to investigate the diagnostic value of diffusion kurtosis imaging (DKI) in benign and malignant breast lesions. At present, Imaging diagnosis of benign and malignant breast nodules mainly focuses on morphology and hemodynamics to reflect the characteristics of lesions. This study intends to reflect the characteristics and changes of microstructure in breast tissues at molecular level by quantitative parameters of DKI, which provides an effective basis for early detection and accurate diagnosis of breast cancer.
Introduction
With the change of lifestyle, the incidence of breast cancer is on the rise[1]. Early detection and treatment are of great significance to reduce the mortality of breast cancer. Diffusion kurtosis imaging (DKI), has shown promise in providing useful information in diagnosis of breast lesions, but the diagnostic performance of DKI needs to be further explored. The purpose of this study was to investigate the diagnostic value of DKI quantitative parameters in benign and malignant breast lesions.Material and Methods
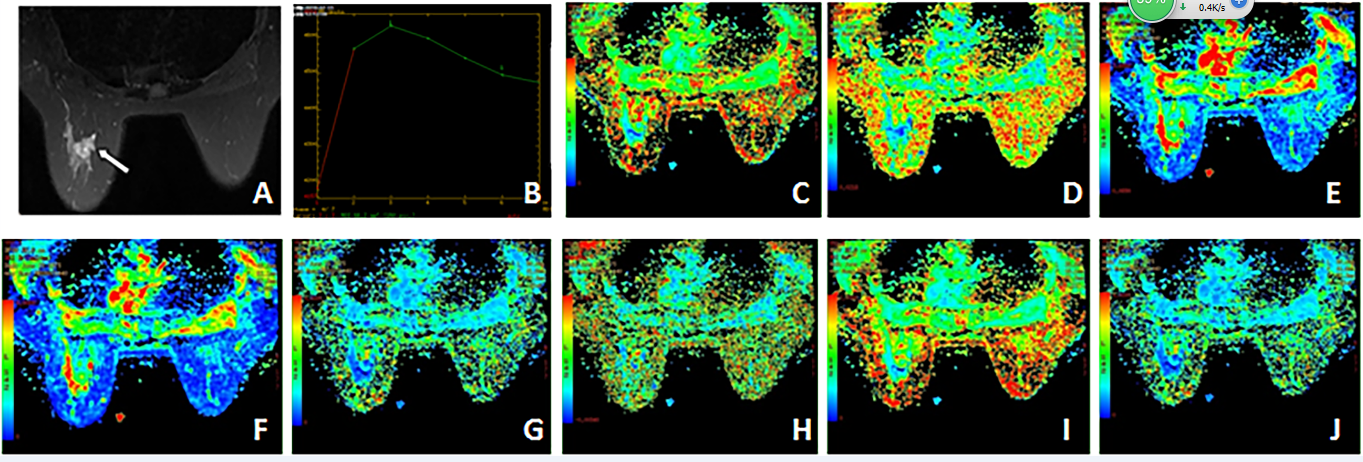
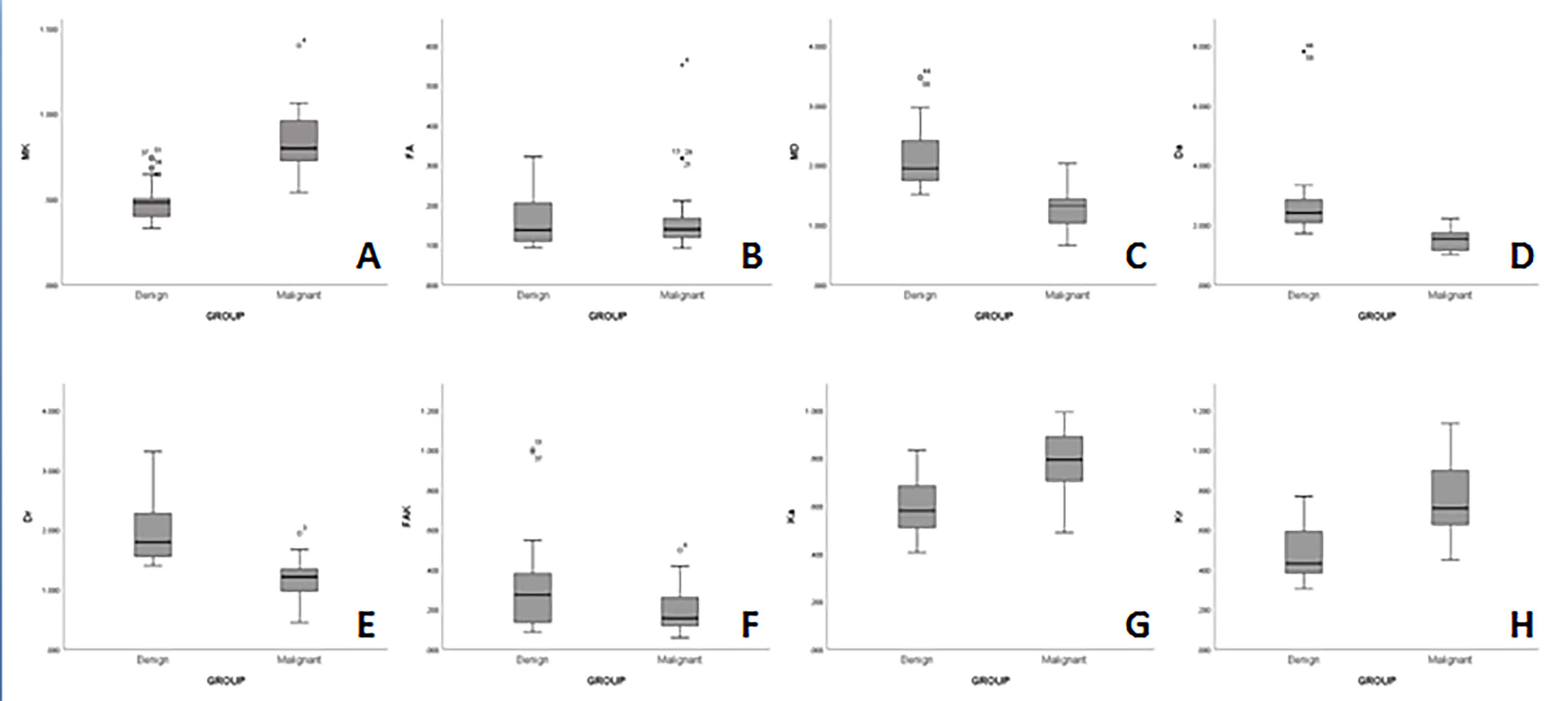
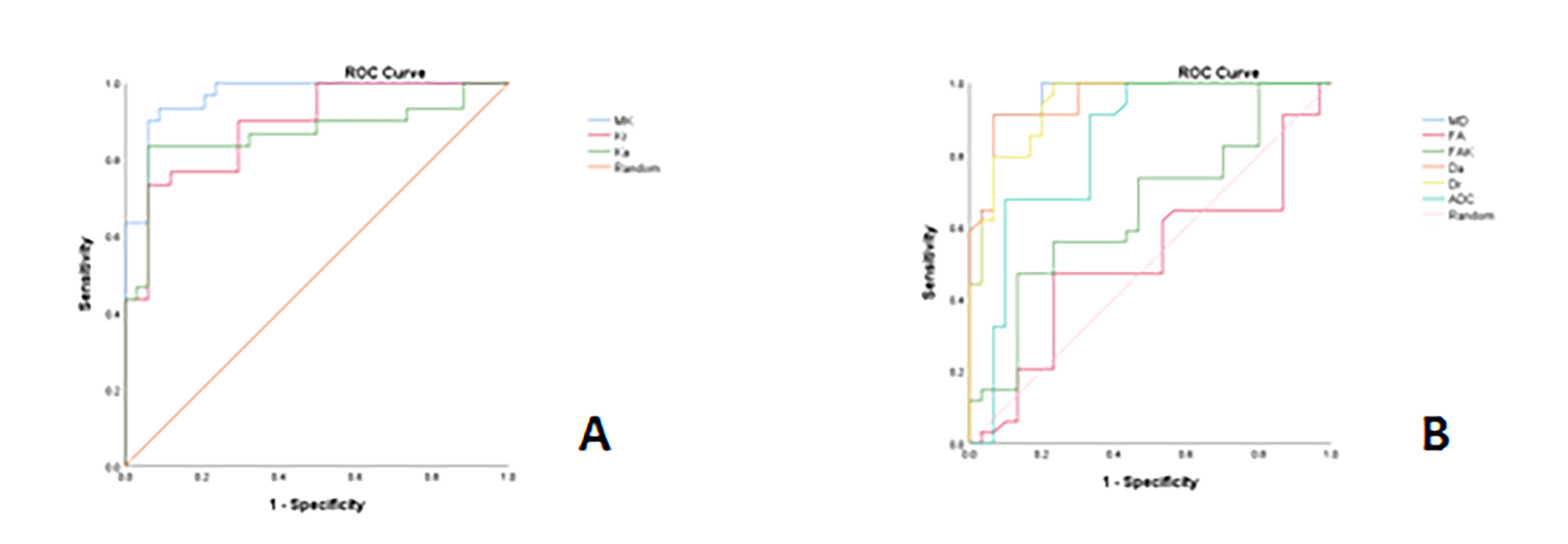
A total of Sixty patients prior to operations were enrolled in this study. Ethical approval and consent forms were obtained. All the subjects underwent MR exams on a 3T MR scanner (Discovery MR750W, GEHealthcare, USA). MR sequences included routine breast sequences as well as DWI (b=0,800s/mm2) and DKI (b=0, 1000, 2000s/mm2 , 15 diffusion directions). Images analyses were performed on GE AW4.6 Workstation by two radiologists, who were blinded to the pathologic results . The ROIs were manually placed on the maximal section of each lesion, carefully to avoid the area of cystic degeneration, necrosis and bleeding. Finally, the DKI parameters including fractional anisotropy(FA), mean diffusivity (MD), axial diffusivity(Da), radial diffusivity(Dr), mean kurtosis(MK), axial kurtosis(Ka), and radial kurtosis(Kr) were measured. 1-sample K-S test and independent sample T-test were applied to investigate the statistical significance of the results. The area under the operating characteristic curve (ROC curve) was calculated to evaluate the diagnostic efficacy of each parameter on benign and malignant breast lesions. The optimal threshold of each parameter and the corresponding youden index, sensitivity and specificity were calculated.Results
Discussion
MRI has been widely used in the diagnosis of breast diseases. DKI, which can reflect the diffusion of tissue water molecules and the complexity of tissue structure, has been investigated for in differentiating benign and malignant breast lesions[2]. The results of this study show that DKI parameters have statistical significance in differential diagnosis of benign and malignant breast lesions. The area under curve (AUC) of these parameters were higher than that of ADC, indicating higher diagnostic efficiency. MK has the highest diagnostic ability and sensitivity among all parameters, and is significantly higher than ADC value. MK is determined by the complexity of ROI structure selected. Compared with benign lesions, breast malignant lesions have more complex microstructure, deviate from Gaussian distribution and higher MK value. Traditional DWI sequence is a single exponential model. Based on the hypothesis of microenvironment homogeneity, it is considered that the diffusion of water molecules in biological tissues follows the Gauss distribution model. In breast cancer, the attenuation of DWI signal with b value does not satisfy the single exponential curve, but is a more complex non-Gauss dispersion form. DKI is a new technique that conforms to the non-Gauss distribution, As a new technology conforming to non-Gauss distribution, DKI can more objectively reflect the diffusion of water molecules in vivo, and can provide relatively real information about the microstructure of tissues[3]. Therefore, compared with traditional DWI, DKI can more accurately reflect the characteristics of microenvironment and water diffusion in tumor, and increase the ability to differentiate between benign and malignant breast lesions.Conclusion
DKI showed better diagnosis efficacy than DWI differential diagnosis of benign and malignant breast lesions.Acknowledgements
No acknowledgement found.References
[1] Sun K,Chen X, Chai W, et al. Breast Cancer: Diffusion Kurtosis MR Imaging-Diagnostic Accuracy and Correlation with Clinical-Pathologic Factors.[J]. Radiology, 2015, 277(1):46-55.
[2] Huang Y, Lin Y, Hu W, et al. Diffusion Kurtosis at 3.0T as an in vivo Imaging Marker for Breast Cancer Characterization: Correlation With Prognostic Factors. [J].J Magn Reson Imaging. 2018 Sep 8.
[3]Li T, Yu T, Li L, et al. Use of diffusion kurtosis imaging and quantitative dynamic contrast-enhanced MRI for the differentiation of breast tumors. [J].J Magn Reson Imaging. 2018 May 2.
Figures