1870
Accelerated T2 Mapping of Breast Cancer Using Compressed Sensing1Radiology, Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2Memorial Sloan Kettering Cancer Center, New York, NY, United States
Synopsis
The use of T2 mapping in the breast is currently limited by prohibitively long acquisition times. We present here a compressed sensing approach and show that we are able to acquire T2 mapping breast images with 5-fold acceleration relative to a fully sampled, multi spin echo sequence. This reduction in acquisition time may make T2 mapping a feasible option for quantitative imaging of the breast, particularly for longitudinal studies such as those evaluating treatment efficacy and response.
Introduction
T2-weighted imaging is routinely used for breast MRI to identify cysts, hemorrhage, necrosis and peritumoral edema, which have prognostic implications1-6. However, signal intensity of T2-weighted images lacks interpretability and reproducibility. This is a particularly problematic for longitudinal imaging studies and biomarker development. Quantitative T2 mapping can be used to overcome this limitation, but existing imaging protocols are too slow for routine clinical use. The purpose of this study is to test a rapid T2 mapping protocol for breast MRI using compressed sensing (CS).Methods
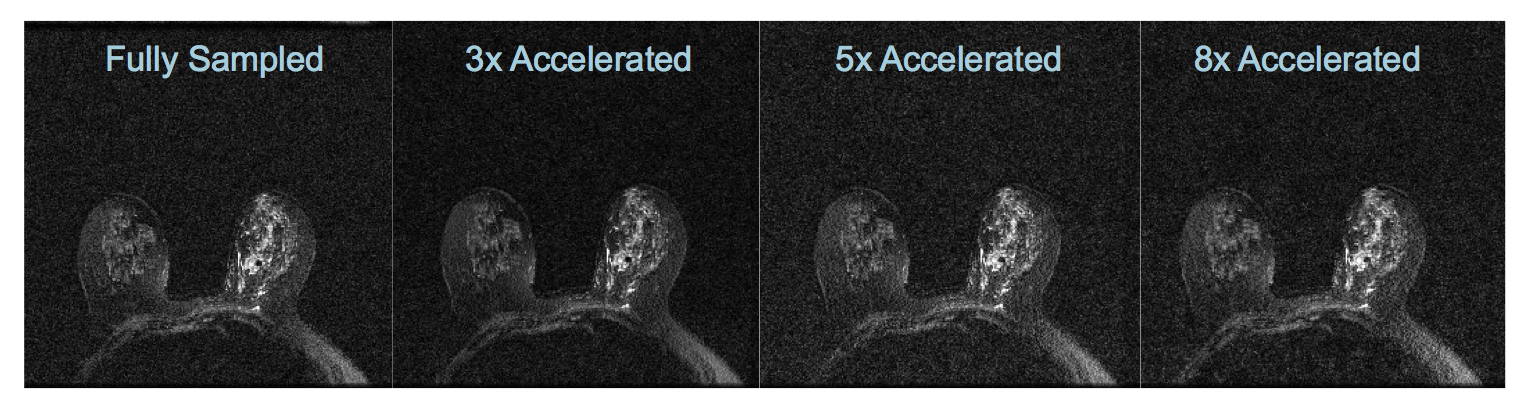
Ten patients with invasive breast cancer were imaged with a product, 2D, T2 mapping sequence employing multi spin echo acquisitions. Relevant imaging parameters included: 16 echoes, multi spin echo, TE=14-228 ms, TR=1.5s, image matrix=300x300, FOV=30x30cm2, slice thickness=1mm, number of slices=5, and scan time=7.5 min. T2 mapping was performed before contrast injection and imaging was done on a 3.0T MR scanner (Discovery 750, GE Healthcare, Waukesha, WI) with an 8- or 16-channel breast coil (Sentinelle by Invivo, Gainesville, FL). Fully sampled k-space was retrospectively undersampled by a factor of 3, 5 and 8 using a varying-density ky-t random undersampling pattern.
A temporal basis set was generated based on a mono-exponential T2 decay signal model for T2 values ranging from 0 to 200 ms. This temporal basis was used to impose a subspace-constrained sparse reconstruction as described by Tamir et al.7, and a locally low-rank constraint was enforced to exploit temporal correlations in the subspace. Image reconstruction was performed using an alternating direction method of multipliers (ADMM) algorithm that is provided in [7].
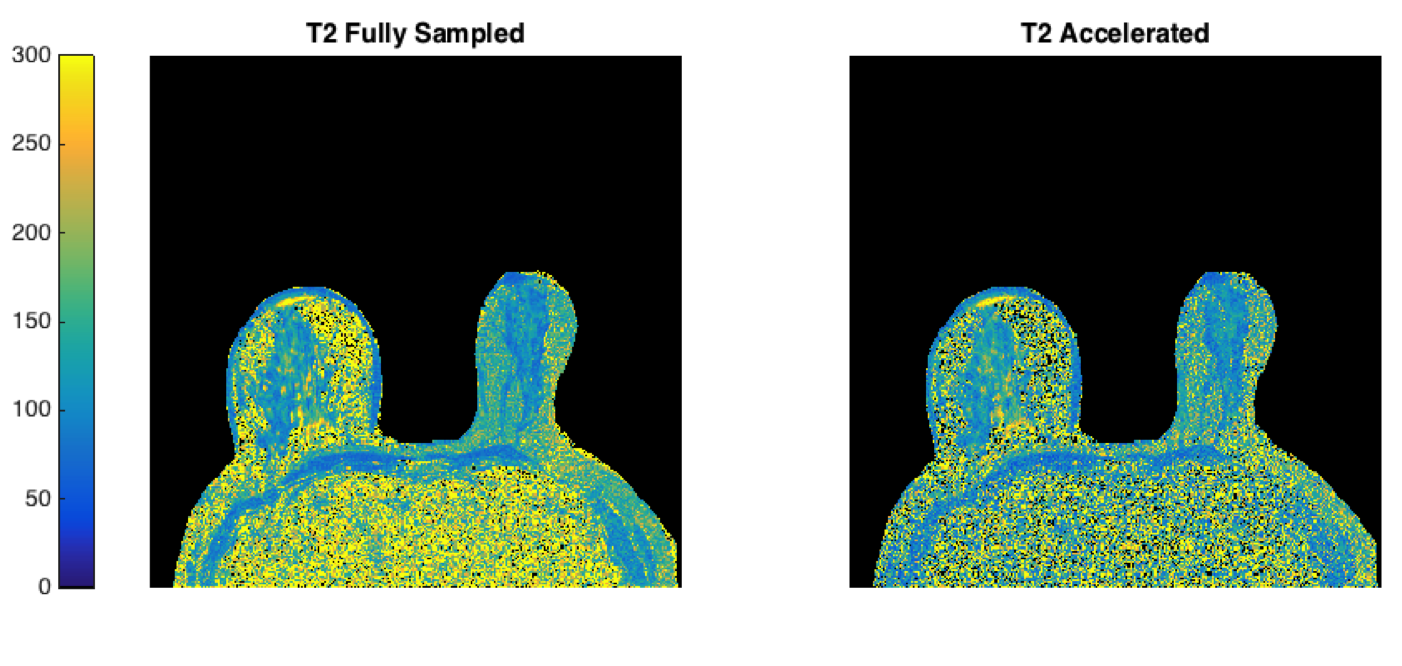
CS accelerated images were compared to fully sampled images. The tumor was segmented on the slice it appeared largest on using the dynamic contrast enhanced, T1-weighted image for reference. T2 maps were generated using a least squares fit to the standard formula S=S(0)exp(-TE/T2) on a pixel-by-pixel basis for both the accelerated and fully sampled data sets, and were compared within the tumor segmentation.
Results and Discussion
Images were accelerated by a factor of 3, 5 and 8 with a maximum root mean square error (RMSE) of 1.5%, 2.2% and 2.3%, respectively (mean across patients 3x = 0.7%, 5x = 0.8%, 8x = 0.9%). Mean structural similarity index (SSIM) was 0.76 for 3x acceleration, 0.74 for 5x acceleration and 0.73 for 8x acceleration. Based on visual assessment, we chose a 5-fold acceleration to be optimal with regard to image fidelity versus acquisition time.
T2 values within the tumor showed a slight bias with higher values from the accelerated sequence (figure 3). The mono-exponential decay model used here is, however, known to have inaccuracies due to indirect and stimulated echoes and we do not claim these values to be correct, but provide them for comparison. This accelerated acquisition can be incorporated into a model-based reconstruction to provide a fast and accurate T2 mapping method in breast8.
Conclusion
We were able to acquire T2 mapping breast images with 5-fold acceleration relative to the fully sampled, multi spin echo sequence. This reduction in acquisition time may make T2 mapping a feasible option for quantitative imaging of the breast, particularly for longitudinal studies such as those evaluating treatment efficacy and response.Acknowledgements
No acknowledgement found.References
1. Westra C, Dialani V, Mehta TS, Eisenberg RL: Using T2-weighted sequences to more accurately characterize breast masses seen on MRI. AJR Am J Roentgenol 2014; 202:W183-90.
2. Moran CJ, Hargreaves BA, Saranathan M, et al.: 3D T2-weighted spin echo imaging in the breast. J Magn Reson Imaging 2014; 39:332–338.
3. Kuhl CK, Klaschik S, Mielcarek P, Gieseke J, Wardelmann E, Schild HH: Do T2‐weighted pulse sequences help with the differential diagnosis of enhancing lesions in dynamic breast MRI? J Magn Reson Imaging 1999.
4. Arponen O, Masarwah A, Sutela A, et al.: Incidentally detected enhancing lesions found in breast MRI: analysis of apparent diffusion coefficient and T2 signal intensity significantly improves specificity. Eur Radiol 2016; 26:4361–4370.
5. Kul S, Oğuz Ş, Eyüboğlu İ, Kömürcüoğlu Ö: Can unenhanced breast MRI be used to decrease negative biopsy rates? Diagn Interv Radiol 2015; 21:287–292.
6. Telegrafo M, Rella L, Stabile Ianora AA, Angelelli G, Moschetta M: Unenhanced breast MRI (STIR, T2-weighted TSE, DWIBS): An accurate and alternative strategy for detecting and differentiating breast lesions. Magn Reson Imaging 2015; 33:951–955.
7. Tamir JI, Uecker M, Chen W, et al. T2 shuffling: Sharp, multicontrast, volumetric fast spin-echo imaging. Magn. Reson. Med. 2017;77(1):180-195.
8. Ben-Eliezer N, Sodickson DK, Block KT. Rapid and accurate T2 mapping from multi-spin-echo data using Bloch-simulation-based reconstruction. Magn. Reson. Med. 2015;73(2):809-817.
Figures