1868
Kaplan-Meier survival curves in breast cancer patients: contributions of nodal volume, tumor volume, residual disease, and response to chemotherapy1Stony Brook University, Stony Brook, NY, United States
Synopsis
The goal of our study was to evaluate whether pre- and post-chemotherapy nodal volume affects the survival profiles of breast cancer patients. In addition, we also evaluated these effects with respect to responders and non-responders to neoadjuvant chemotherapy. Comparison was made by analyzing the effects of tumor volume on survival profiles. We concluded that recurrence-free survival profile is dependent on axillary lymph node volume, and that non-responder patients with large nodes may need more vigorous treatment and follow up as they were associated with worse recurrence-free survival.
Introduction
Survival profiles in breast cancer patients have been studied in association with different imaging and pathological parameters, such as tumor volume and pathological complete response (PCR). Smaller tumor volume at both early and post-neoadjuvant chemotherapy time points is linked to more favorable recurrence-free survival (RFS) with hazard ratios of 1.02 and 1.07 (p<0.001), respectively [1]. PCR is controversial, with some studies showing PCR not affect RFS (p=0.12) [1] and other showing responders having a better survival profile with a hazard ratio of 0.29 (p=0.02) [2].
The contribution of axillary lymph node (aLN) MRI volume to survival curve profiles has not been investigated. The goal of our study was to evaluate whether pre- and post-chemotherapy nodal volume affects the survival profiles of breast cancer patients. In addition, we also evaluated these effects with respect to responders and non-responders to neoadjuvant chemotherapy. Comparison was made by analyzing the effects of tumor volume on survival profiles.
Methods
This study included 92 stage-2 or 3 breast-cancer patients [3] with affected ipsilateral aLNs. aLNs were segmented on the first post-contrast 1.5T MRI (1x1x2mm). Nodal and tumor volumes pre- and post-NAC were separated into large and small groups to compare recurrence-free survival profiles. Kaplan Meier survival curves were separated by full, breast and nodal PCR. Log-rank test was used to compare two groups and hazard ratio (HR) was calculated. Sample sizes across groups vary slightly based on availability of outcome measures (PCR and/or RFS).
For consistency, only largest node per patient was analyzed. Average volume of unaffected contralateral aLNs was 0.56±0.54 cc (198 normal nodes). Threshold of 3mL was applied to separate into large and small nodes pre-NAC; 40.2% of patients had large aLNs pre-NAC
Average pre-NAC tumor volume was 25.8±23.7cc. Threshold of 36cc was used; 29.8% of patients had large volume at pre-NAC time point. Unlike nodal volume, pre-NAC tumor distribution was broad and using a higher threshold would result in too few samples in large group.
Post-NAC, nodal threshold was 0.8SD of normal node size, given that aLNs shrunk appreciably; 22.2% of patients had large nodes post-NAC. Post-NAC tumor volume was separated into residual and no-residual enhancing tumor to mimic radiological complete response; 72.0% of patients had residual enhancing disease. Although these thresholds were arbitrary they enabled investigation of effects of node and tumor size on survival curves.
Results
Results separating by post-NAC pathology are shown in Figure 1 and Table 1. Survival curves were not different between complete responders (p=0.15) or breast responders (p=0.12). However, they were different based on nodal response (p=0.01) with nodal non-responders being over twice as likely to have recurrence.
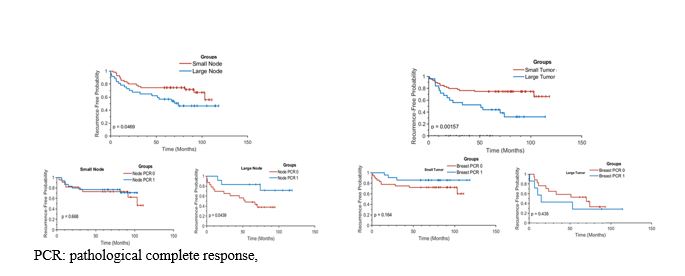
Results separating into large and small nodes and tumor volumes pre-NAC, followed by their respective pathological status are summarized in Figure 2 and Table 2. Separating into large and small node or tumor volumes resulted in significantly different survival curves (p<0.05), but further separation into PCR was only informative for large nodes (p=0.04), where large node non-responders were over 3 times as likely to have a recurrence.
Results separating into large and small nodes and tumor volumes post-NAC, followed by their respective pathological status are summarized in Figure 3 and Table 3. RFS was not dependent on whether or not patient had residual enhancing tumor volume (p=0.35), but was dependent on large/small node separation (p=0.03). Similar to above, the large node non-responder was more likely to have a recurrence, specifically 6 times more likely.
Discussion
A major finding of this study is that nodal volume at both pre and post NAC affects survival curves. Specifically, patients with larger nodes having worse survival curve (pre-HR:0.52, p=0.05; post-HR:0.48, p=0.04). This trend has been noted in other cancers such as lung (pre-HR: 1.03, p=0.02; post-HR: 1.05, p=0.02) [4] and head/neck [5], but not in breast cancer. Further separation by responders versus responders highlighted the importance of large nodes to achieve PCR post-treatment. This information is clinically relevant and likely influences patient management post-NAC.Conclusion
Recurrence-free survival profile is dependent on lymph node size. Our findings suggest that non-responder patients with large nodes may need more vigorous treatment and follow up as they were associated with worse recurrence-free survival. To our knowledge, this is the first study that investigated the contribution of axillary lymph node volume to recurrence-free survival curves in breast cancer patients.Acknowledgements
No acknowledgement found.References
[1] Hylton NM et al. Neoadjuvant Chemotherapy for Breast Cancer: Functional Tumor Volume by MR Imaging Predicts Recurrence-free Survival-Results from the ACRIN 6657/CALGB 150007 I-SPY 1 TRIAL. Radiology. 2016 Apr;279(1):44-55. doi: 10.1148/radiol.2015150013. Epub 2015 Dec 1.
[2] Esserman LJ et al. Pathologic complete response predicts recurrence-free survival more effectively by cancer subset: results from the I-SPY 1 TRIAL--CALGB 150007/150012, ACRIN 6657. J Clin Oncol. 2012 Sep 10;30(26):3242-9. doi: 10.1200/JCO.2011.39.2779. Epub 2012 May 29.
[3] Hylton NM et al. Locally advanced breast cancer: MR imaging for prediction of response to neoadjuvant chemotherapy--results from ACRIN 6657/I-SPY TRIAL. Radiology. 2012 Jun;263(3):663-72. doi: 10.1148/radiol.12110748.
[4] Agrawal V et al. Lymph node volume predicts survival but not nodal clearance in Stage IIIA-IIIB NSCLC. PLoS One. 2017 Apr 20;12(4):e0174268. doi: 10.1371/journal.pone.0174268. eCollection 2017.
[5] Lodder WL et al. Prognostic significance of radiologically determined neck node volume in head and neck cancer: a systematic review. Oral Oncol. 2012 Apr;48(4):298-302. doi: 10.1016/j.oraloncology.2011.11.001. Epub 2011 Nov 22.
Figures