1866
Morphology of Breast lesions on Ultrafast Dynamic Contrast Enhanced MRI using Compressed Sensing Reconstruction1Diagnostic Imaging and Nuclear Medicine, Kyoto University, Kyoto, Japan, 2Kyoto University Graduate School of Medicine, Kyoto, Japan, 3MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 4Breast Surgery, Kyoto University, Kyoto, Japan, 5Diagnosti c Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan
Synopsis
Using ultrafast DCE (UF-DCE) MRI with compressed sensing reconstruction, size and morphology of breast lesions on very early phase images within 1 minutes post contrast injection were compared to those on conventional DCE (C-DCE) MRI. The size of the lesions was slightly smaller on UF-DCE but within-2mm difference in approximately 80 % of the lesions. Morphological evaluations were the same in approximately 80% of the lesions yet irregular margin and clustered ring on C-DCE MRI may not be reflected to the appearance on UF-DCE, which should be noted in interpreting lesions using UF-DCE.
Introduction:
Ultrafast DCE (UF-DCE) MRI is a promising method of evaluating breast lesions with much shorter image acquisition. High temporal resolution (4~8 sec) with 1 mm in-plane resolution can be achieved. In-flow kinetic information can be evaluated using new semi-quantitative parameters including maximum slope. Diagnostic performance of kinetic information using these semi-quantitative UF-DCE parameters are equivalent to conventional kinetic information obtained on conventional DCE (C-DCE) MRI protocols (1-4). On the other hand, evidence on morphology is limited. Image quality and spatial resolution of UF-DCE using compressed sensing seems to be better than that using view-sharing technique (5). In order to replace C-DCE MRI with UF-DCE MRI, difference of morphological information between the two protocols should be carefully examined. Difference in temporal resolution and timing from the injection of contrast agent may affect the morphological evaluation. In this study, we aimed to compare size and BI-RADS 2013-based morphological assessment of the lesion on UF-DCE MRI using compressed sensing to the assessment on C-DCE MRI.Material and Methods:
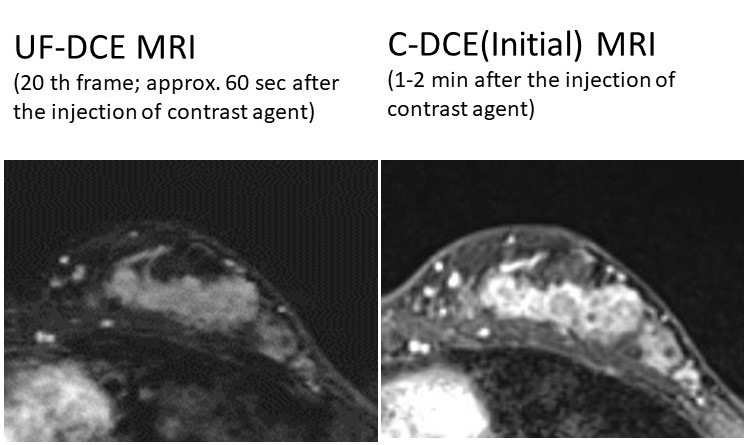
Study population consists of 74 consecutive patients with 104 lesions who underwent Breast MRI with UF-DCE protocol to evaluate suspicious/known breast lesions from April 2016 to May 2018 with corresponding histopathological diagnosis. MR scanning was performed using a 3 T MR system (MAGNETOM Prisma/Skyra, Siemens Healthcare, Erlangen, Germany) equipped with a dedicated 18/16-channel bilateral breast array coil. T2-weighted, T1-weighted, diffusion weighted and fat-suppressed T1-weighted DCE images were obtained. C-DCE Protocol: Fat-suppressed T1-weighted DCE images were obtained as follows: pre-contrast and two post-contrast acquisitions at 1–2 (Initial phase) and 5–6 min (delayed phase) after gadolinium injection for whole breast axial scanning with high temporal resolution (3D-VIBE: TR/TE 3.70/1.36ms, FA 15 and FOV 330 ×330 mm2, matrix 384x269, thickness 1.0 mm, TA 1min), post contrast acquisition at 2–5 min after gadolinium injection for whole breast coronal scanning with high spatial resolution (3D-VIBE: TR/TE 4.01/1.63ms, FA 15, FOV 330×330 mm, matrix 512x461, TA 2.5min thickness 0.8mm). Infused gadolinium contrast materials were gadobutrol (Gadovist, Bayer, Germany) at a dose of 0.1 ml/kg power injected at a speed of 2.0 ml/s and flushed with 20 ml at a speed of 2.0 ml/s of saline at the same rate. UF-DCE Protocol: Acquisitions were obtained using a prototype sequence based on the 3D gradient-echo VIBE sequence at a very early phase (between pre-contrast and initial phase of C-DCE protocol), starting 15 seconds before injection and lasting until 1 min after gadolinium injection (TR/TE 5.0/2.5, FA 15, FOV 360 ×360 mm, matrix 384x269, thickness 2.5 mm ,CS acceleration=16.5, temporal resolution 3.7 sec for 20 time frames). CS reconstruction was conducted with 30 iterations. Image analysis was performed per lesion. Two or more lesions from one patient were included if the corresponding histopathological diagnosis were available. On UF-DCE MRI, all 20 images of different time frames were reviewed to identify enhancing lesions. For identified lesions, their size (maximum diameter) and morphology (mass and non-mass enhancement (NME), shape, margin, and internal enhancement characteristic) were evaluated by an experienced radiologist based on BI-RADS MRI 2013. On C-DCE MRI,initial phase DCE images (1-2 min post contrast) were used to evaluate the same lesion. Lesion size between UF-DCE and C-DCE MRI was compared using Wilcoxon’s signed rank test.Results:
In total 104 enhancing lesions (76 mass: 28 NME, 77 malignant and 27 benign lesions) were identified. Mean lesion size on UF-DCE MRI was 23.6mm, slightly smaller than the size on C-DCE MRI (25.1 mm: p<0.001) Lesion size was within 2mm-difference in 80/104 lesion (77%). Difference tended to be more obvious among malignant lesions than among benign lesions (p<0.001 vs p=0.045: fig.1). Morphological evaluations were summarized in Table 1&2. For 76 mass lesions, morphological evaluations were identical between UF-DCE and C-DCE in approximately 80%. Morphological discrepancy was most frequently observed in margin. The most frequently observed difference were “circumscribed” margin on UF-DCE. For 28 NME lesions, the most discrepant morphology was “clustered ring”.Representative cases with discrepant findings are shown in fig.2&3.Discussion & Conclusions:
Size and morphology of breast lesions were equivalent in approximately 80% of lesions. Lesion size tended to be slightly smaller on UF-DCE. Morphologically, irregular margin of the mass and clustered ring of NME on C-DCE MRI may not be reflected on UF-DCE MRI. This could be explained by the different timing of the scan. Contrast agent might not reach the peripheral area of the lesion in the very early phase. Although imaging findings are similar in UF-DCE in most of the cases, he above discrepancies should be noted when interpreting UF-DCE MRI. Our analysis may indicate the need for further protocol optimization of CS protocol in terms of morphology as well as kinetics.Acknowledgements
We thank Dr.Katsutoshi Murata and Yuta Urushibata, Siemens Japan, for their technical support in this work. This work was partly supported by Grant-in-Aid for Scientific Research on Innovative Areas “Initiative for High-Dimensional Data-Driven Science through Deepening of Sparse Modeling”, and Grant-in-Aid for Scientific Research (C) “Evaluation of Wash in Phase using Ultrafast MRI of the Breast.References
1) Mann RM et al. A novel approach to contrast-enhanced breast magnetic resonance imaging for screening: high-resolution ultrafast dynamic imaging. Invest Radiol 2014; 49:p579 2) Abe H, et al., Kinetic analysis of benign and malignant breast lesions with ultrafast dynamic contrast-enhanced MRI: comparison with standard kinetic assessment. AJR Am J Roentgenol, 2016. 207(5): p1159. 3) Goto M, et al., Diagnostic performance of initial enhancement analysis using ultra-fast dynamic contrast-enhanced MRI for breast lesions. Eur Radiol, 2018. 4) Onishi N et al. Ultrafast dynamic contrast-enhanced MRI of the breast using compressed sensing: separate visualization of breast arteries an veins. JMRI 2017 5) Vreemann S et al. Compressed sensing for breast MRI: resolving the trade-off between spatial and temporal resolution. Invest Radiol 2017Figures
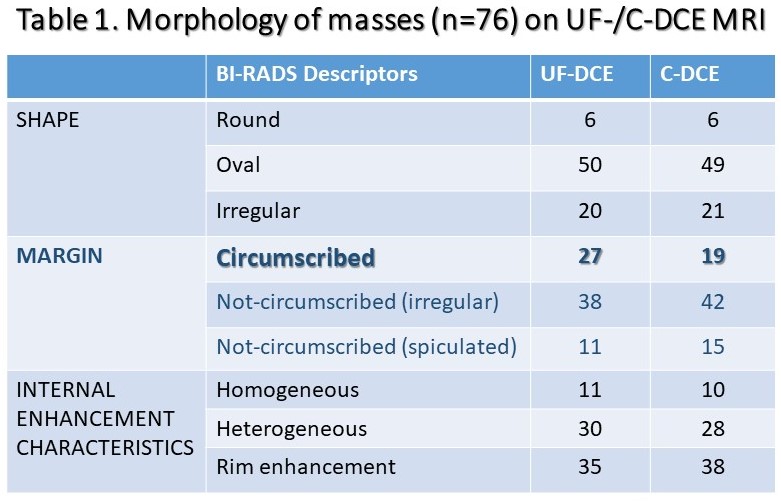
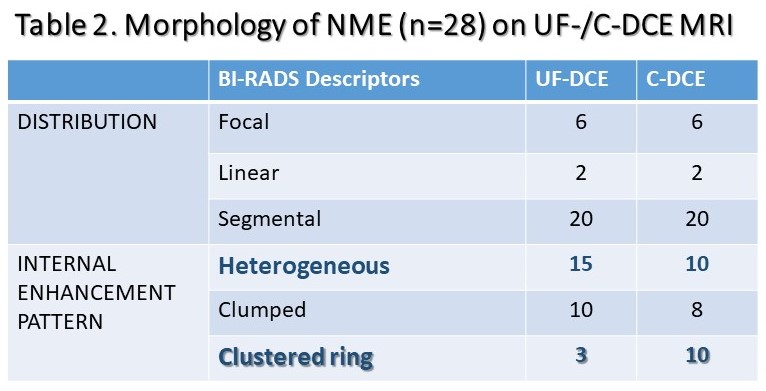
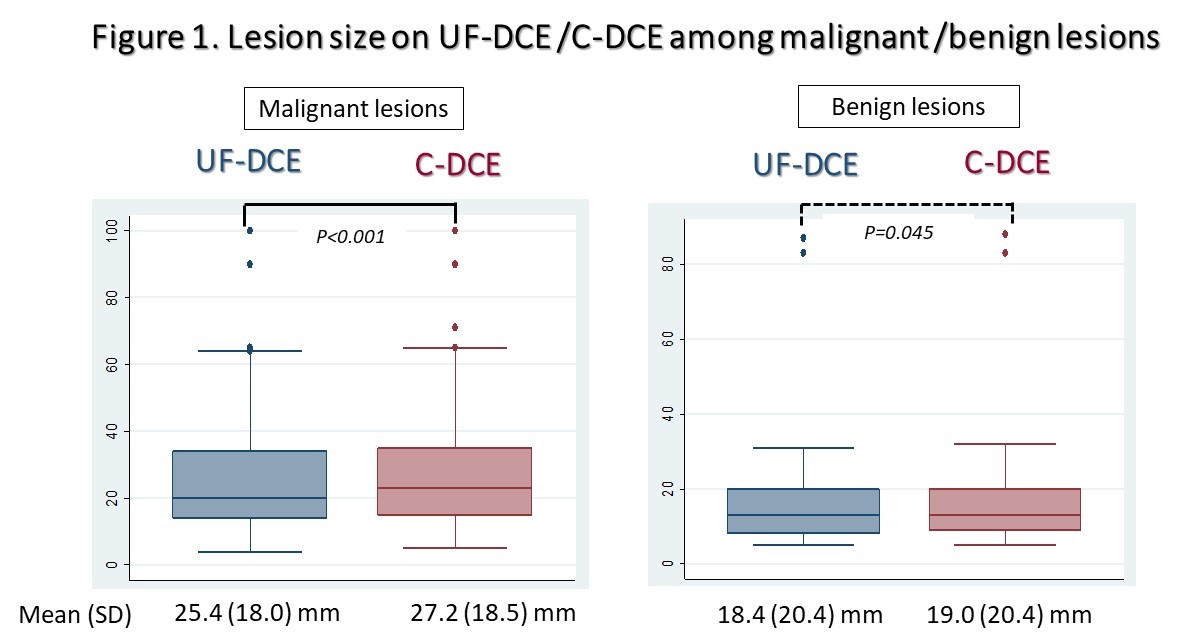
Figure 1.Comparison of lesion size on UF-DCE and C-DCE MRI among malignant (Lt) and benign (Rt) lesions. Lesion size is significantly smaller on UF-DCE. The difference is more obvious among malignant lesions (p<0.001) than among benign lesions (p=0.045)