1859
Multiband SENSE accelerated diffusion weighted imaging with CAIPIRINHA: Preliminary study of clinical utility in the breast1Radiology, University of Washington, Seattle, WA, United States, 2Philips Healthcare, Gainesville, FL, United States
Synopsis
Advanced DWI techniques necessitate acquisition of a large number of image slices such as to obtain a greater number of b values for IVIM or more gradient directions for DTI. These increase the acquisition time, making it difficult to incorporate advanced techniques within the clinical workflow. The purpose of this study was to examine the utility of MB-SENSE acceleration for reducing scan times of breast DWI. Our qualitative and quantitative assessments showed MB-SENSE could dramatically reduce scan time without reducing image quality and accuracy of lesion ADC measures in breast DWI.
Introduction
Diffusion Weighted Imaging (DWI) measures the Brownian motion of water molecules and provides quantitative information on tumor cellularity and microstructure. DWI is increasingly being utilized as a non-contrast imaging technique to detect and characterize breast lesions1. However, the need to acquire multiple slices to cover both breasts fully, multiple b-values to accurately calculate ADC, and multiple signal averages to improve signal-to-noise (SNR), all lengthen scan time. Longer scan times can result in detrimental effects from patient motion and limits the clinical feasibility of more advanced DWI approaches. Multiband2 SENSE (MB-SENSE) is a fast imaging technique that allows simultaneous excitation of multiple slices. DWI has benefited greatly from multiband imaging in the brain but there is a dearth of data regarding its performance in breast imaging. The purpose of the study was to examine the feasibility of Multiband SENSE accelerated DWI3,4 (mbDWI) for breast imaging and to perform quantitative and qualitative comparisons with a standard clinical DWI EPI sequence (cDWI).Methods
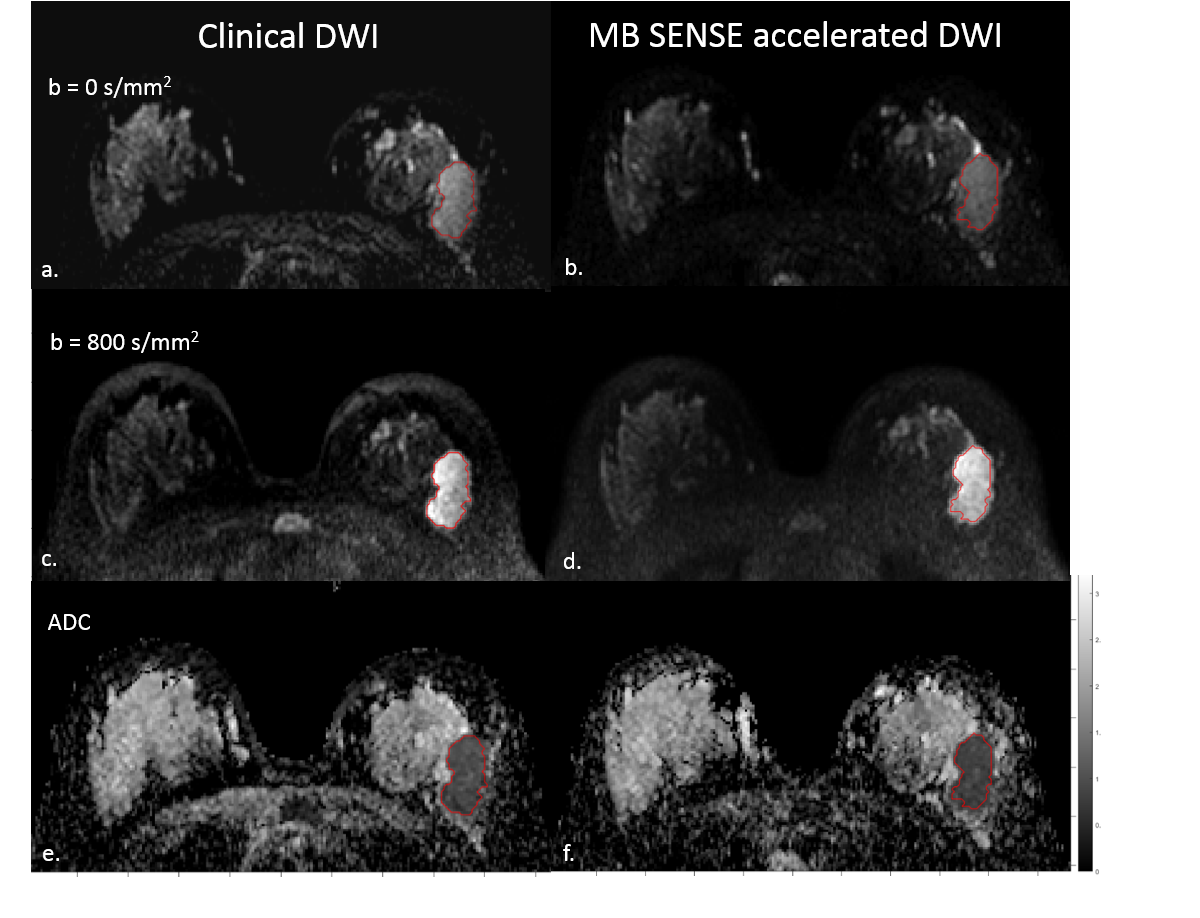
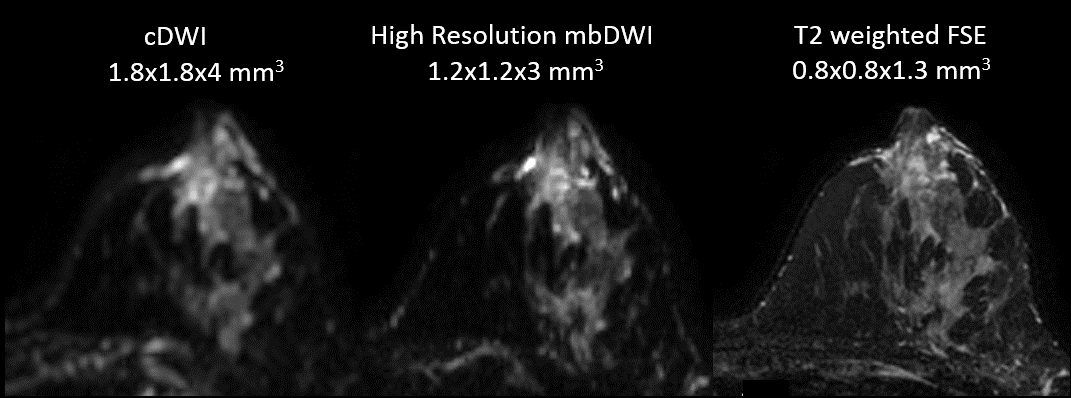
After IRB approval, 20 patients with breast cancer (median age: 55 years range: 28-83 years) undergoing MRI to evaluate the extent of disease were enrolled to undergo an additional mbDWI scan during their exam. MRI acquisitions were performed on a 3T clinical scanner (Achieva, Philips Healthcare, Best, The Netherlands) using a 16-channel breast coil. The cDWI sequence was acquired as reference, with: TR/TE=5043/60 ms, echo train length=67, FOV=360x360mm2, voxel size=1.8x1.8x4mm3, NSA=2, in plane SENSE factor=3, SPAIR with gradient reversal fat suppression, b=0/100/600/800/1000 s/mm2, high-b-averaging=on, 30 slices, and 4:33 min scan time. The mbDWI sequence was acquired with the same parameters as cDWI, except: TR/TE = 3500/80ms, b=0/100/800/1500/2500 s/mm2, MB-SENSE factor=2, FOV/2 CAIPIRINHA2 shift, and 3:33 min scan time. We additionally explored the utility of mbDWI to increase spatial resolution to 1.2x1.2x3 mm3 using the same protocol as mbDWI except b=0/800 s/mm2, 40 slices, and 1:45min scan time. Apparent Diffusion Coefficient (ADC) maps of cDWI and mbDWI were generated with b=0/100/800 s/mm2 for both sequences using voxel-by-voxel monoexponential fit. Lesion ADC values were calculated separately for cDWI and mbDWI and compared using paired Wilcoxon signed-rank test. For qualitative assessments, an experienced radiologist compared cDWI vs. mbDWI in terms of image quality and presence of artifacts or other issues using the following scoring method: 0 = equal image quality, +1 = mbDWI higher image quality, -1 = cDWI higher image quality.Results
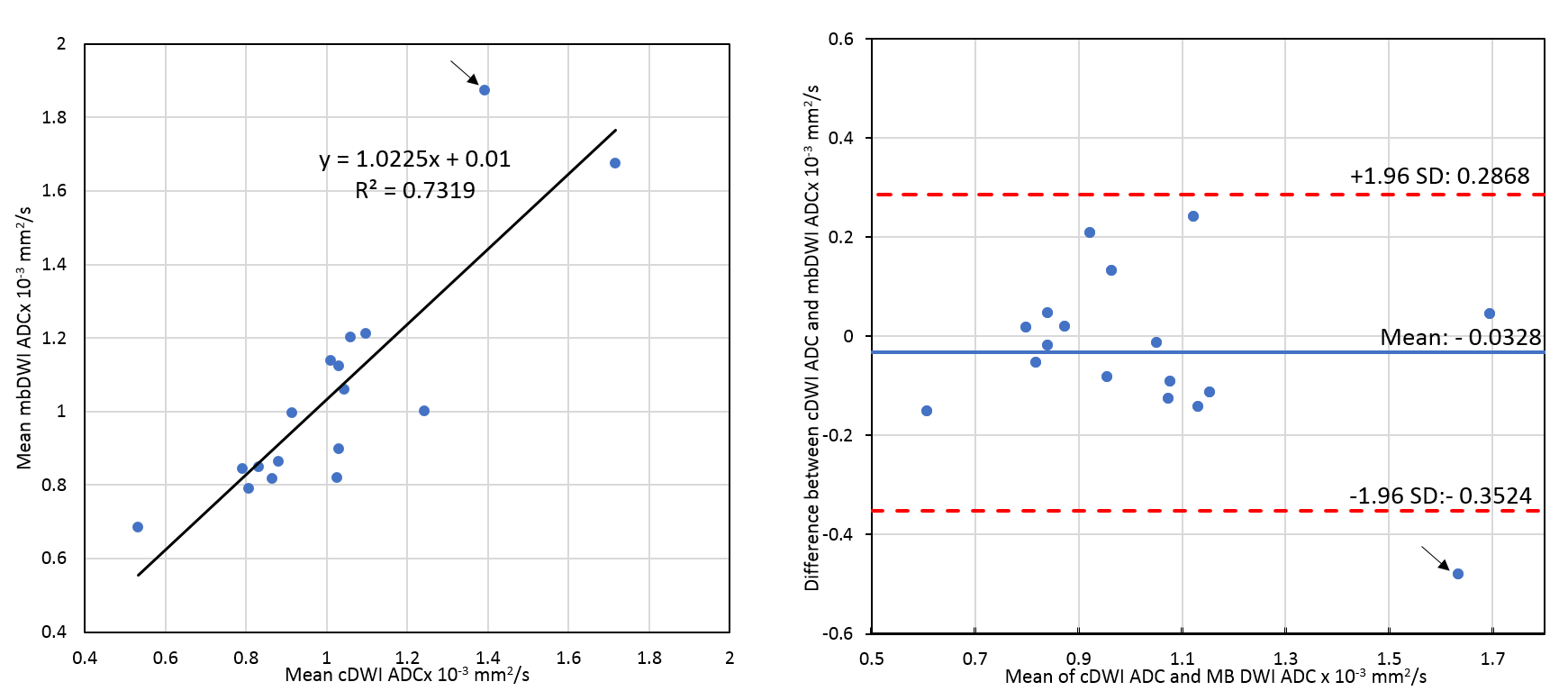
Of the 20 patients who underwent mbDWI, 16 had invasive ductal carcinoma, 3 invasive lobular carcinoma, and 1 DCIS. Lesions ranged in size from 7 to 77mm (median, 21.5mm). An example case is shown in Fig1. Quantitative analysis in 17/20 patients (lesions in three patients could not be measured due to significant biopsy artifacts) showed no significant difference in lesion ADC measures for cDWI (median=1.01mm2/s, range =0.53-1.71mm2/s) vs. mbDWI (median=0.99mm2/s, range=0.68-1.87mm2/s, p = 0.49), Fig2. Radiologist qualitative assessment demonstrated equal (score 0, N = 1) or better (score +1, N = 19) image quality for mbDWI than cDWI, with no cases where mbDWI quality was worse than cDWI (score -1). In the 19 cases where mbDWI was assessed as having higher image quality, reasons noted were less distortion (8 cases), better fat suppression (9 cases), higher SNR (7 cases) and less artifacts (4 cases).
MbDWI enabled dramatic (~50%) reduction in TR and/or number of slices that could be collected during a given scan time, with little tradeoff in image quality. For our study, we fixed TR for mbDWI at 3500ms in order to maintain adequate SNR, although minimum TR possible was 3016 ms, which could have reduced scan time even further. MbDWI showed excellent utility to increase slice coverage for high spatial resolution DWI acquisitions (Fig 3).
Discussion and Conclusion
This study demonstrated that mbDWI can be used to speed up acquisitions without compromising image quality and fidelity of quantitative ADC measurements. Of note, radiologist assessment found image quality preferable with mbDWI in most cases, although the reasons for the differences are not entirely clear and may relate to differences in TR and TE, requiring further investigation. By shortening scan durations, MB-SENSE increases the clinical feasibility of performing advanced breast DWI acquisitions involving a larger number of slices such as to achieve higher spatial resolution with thinner slices, intravoxel incoherent motion (IVIM) and kurtosis modeling with more b values, or diffusion tensor imaging (DTI) with more gradient directions.Acknowledgements
Supported by NIH/NCI research grant R01CA207290 and in-kind support from Philips Healthcare.References
- Partridge SC, Nissan N, Rahbar H, et al. Diffusion-Weighted Breast MRI: Clinical Applications and Emerging Techniques. J Magn Reson Imaging. 2017;45, 337-355.
- Setsompop K, Gagoski BA, Polimeni JR, et al. Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty. Magn Reson Med. 2012;67, 1210-1224
- Taviani V, Alley MT, Banerjee S, et al. High-resolution diffusion-weighted imaging of the breast with multiband 2D radiofrequency pulses and a generalized parallel imaging reconstruction. Magn Reson Med. 2017;77, 209-220
- Filli L, Ghafoor S, Kenkel D, et al Simultaneous multi-slice readout-segmented echo planar imaging for accelerated diffusion-weighted imaging of the breast. European Journal of Radiology 85 (2016) 274-278
- Nguyen VT, Rahbar H, Olson ML, et al. Diffusion Weighted Imaging: Effects of Intravascular Contrast Agents on Apparent Diffusion Coefficient Measures of Breast Malignancies at 3T. J Magn Reson Imaging. 2015; 42(3): 788-800
Figures