1854
One millimeter isotropic breast DWI combining readout-segmented EPI, super-resolution and simultaneous multi-slice acceleration: validation in a diffusion/resolution phantom and volunteers.1IADI, INSERM U1254 and Université de Lorraine, Nancy, France, 2Laboratoire de Recherche en Imagerie INSERM / Université Paris Descartes, Sorbonne Paris Cité, PARCC UMR 970, Faculté de médecine, Paris, France, 3CIC-IT 1433, INSERM, CHRU de Nancy and Université de Lorraine, Nancy, France
Synopsis
The low resolution of diffusion-weighted imaging (DWI) is the main limiting factor in screening breast MRI. Recently a method was proposed for one millimeter isotropic DWI covering the entire breasts. Based on a readout-segmented DW-EPI sequence, 3 stacks of thick slices (3 mm) are acquired with 1mm-shifts in the slice direction; then a 1x1x1 mm3 dataset is obtained using a super-resolution reconstruction (SRR). In this study we further validate the method using a commercial diffusion breast phantom, in terms of SNR, resolution and ADC values. Additionally, SMS acceleration is investigated to reduce the total scan time below 10 min.
Introduction
High-resolution diffusion-weighted imaging (DWI) is very effective in the characterization and detection of breast tumors (1). However, high resolution (HR) DWI is challenging due to the long readout direction along the breasts (right-left), which yields images with low signal-to-noise ratio (SNR) and prone to susceptibility artifacts. Recently an acquisition scheme was proposed using three readout-segmented EPI (rs-EPI) (2) scans with 1x1x3 mm3 resolution, with 1mm-shifts in the slice direction, followed by super-resolution reconstruction (SRR) to obtain isotropic 1x1x1 mm3 DWI datasets (3). This protocol was shown to provide a large SNR boost compared to native 1x1x1 mm3 scan, with minimal loss of spatial resolution. The aim of the present work is two-fold: (i) further validate the spatial resolution, SNR and ADC values obtained by SRR (with/without SMS) using a commercial breast diffusion phantom; (ii) optimize this DWI protocol using a simultaneous multi-slice (SMS) technique (4).Methods
Data acquisition
Breast MRI examinations were performed using a 3T clinical MR scanner (MAGNETOM Prisma; Siemens Healthcare, Erlangen, Germany), with dedicated 18-channel breast array coil. The unaccelerated SRR protocol (without SMS) was comprised of three sets of rs-EPI low resolution (LR) axial images aquired with 1 mm shifts at each repetition (whole breasts coverage, 1x1x3 mm3, b = 0, 200, and 800 s/mm2; 50 slices, TR/TE=10410/56ms, FOV 320x160mm2). It was applied to eight healthy subjects and a breast diffusion phantom (High Precision Devices Inc, Boulder, USA). The SMS accelerated protocol was set with a prototype SMS-rs-EPI. Parameters were the same, except slice acceleration=2, TR/TE=5440/60ms (TR had to be shortened since the number of excited slices is halved with SMS), and FOV 320x162mm2. It was applied to one healthy subject and the breast diffusion phantom.
Reconstruction and data analysis
Reconstruction of isotropic volumes (1x1x1 mm3) was performed for both rs-EPI and SMS-rs-EPI using SRR with Beltrami regularization (3). ADC maps were calculated using the 3 b values, by linear fitting the logarithmic relative intensity against b0. In the phantom, six regions of interest (ROI) were drawn to extract the different compartments with known ADC. Furthermore, spatial resolution was assessed visually using the cylinder compartments with varying radii. Finally, SNR was calculated using the double acquisition method (using the sum and subtraction of two SRR images), with an ROI drawn in a homogeneous area (i.e. with small variation in noise level) (5):
$$SNR = \frac{Signal_{ mean ROI}}{\sigma_{ROI}}$$
$$Signal_{ mean} = \frac{mean (S_1+S_2)_{ROI}}{2}$$
$$\sigma_{ mean} = \frac{\sigma(S_1-S_2)_{ROI}}{\sqrt{2}}$$
In the subjects, ADC values were obtained from carefully drawn ROIs in left and right breast, selecting a region with no fatty tissue and showing a texture characteristic of normal fibroglandular tissues.
Results
The total acquisition time of three acquisitions with/without SMS acceleration was 9:36 min/15:42 min.
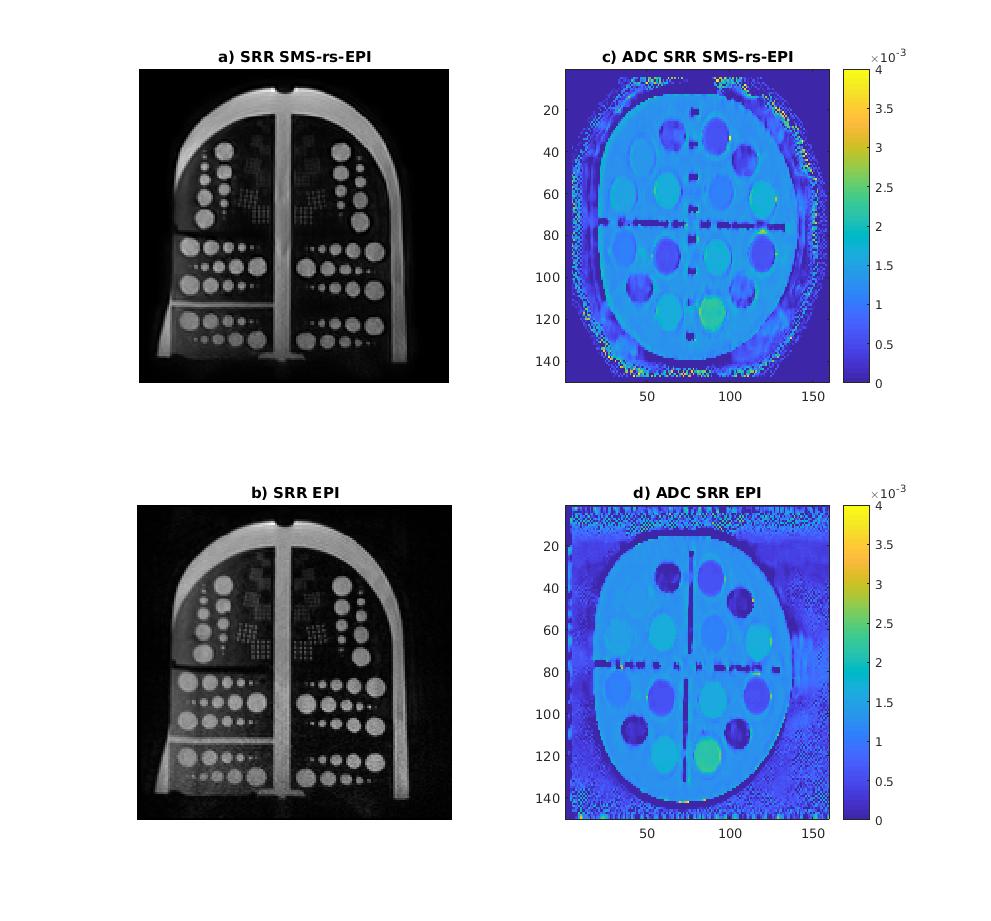
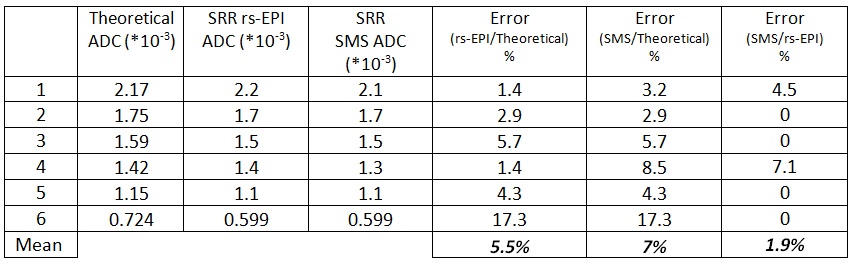
Figure 1 shows the reconstructed phantom data, including the spatial resolution patterns and the diffusion compartments with varying ADC values. Table 1 shows the theoretical and measured ADC values in the phantom with/without SMS. The difference in ADC values was 1.9% between the unaccelerated SRR protocol and its SMS-accelerated version. Table 2 shows signal, noise and SNR with the two protocols. A minor reduction of SNR is obtained with SMS.
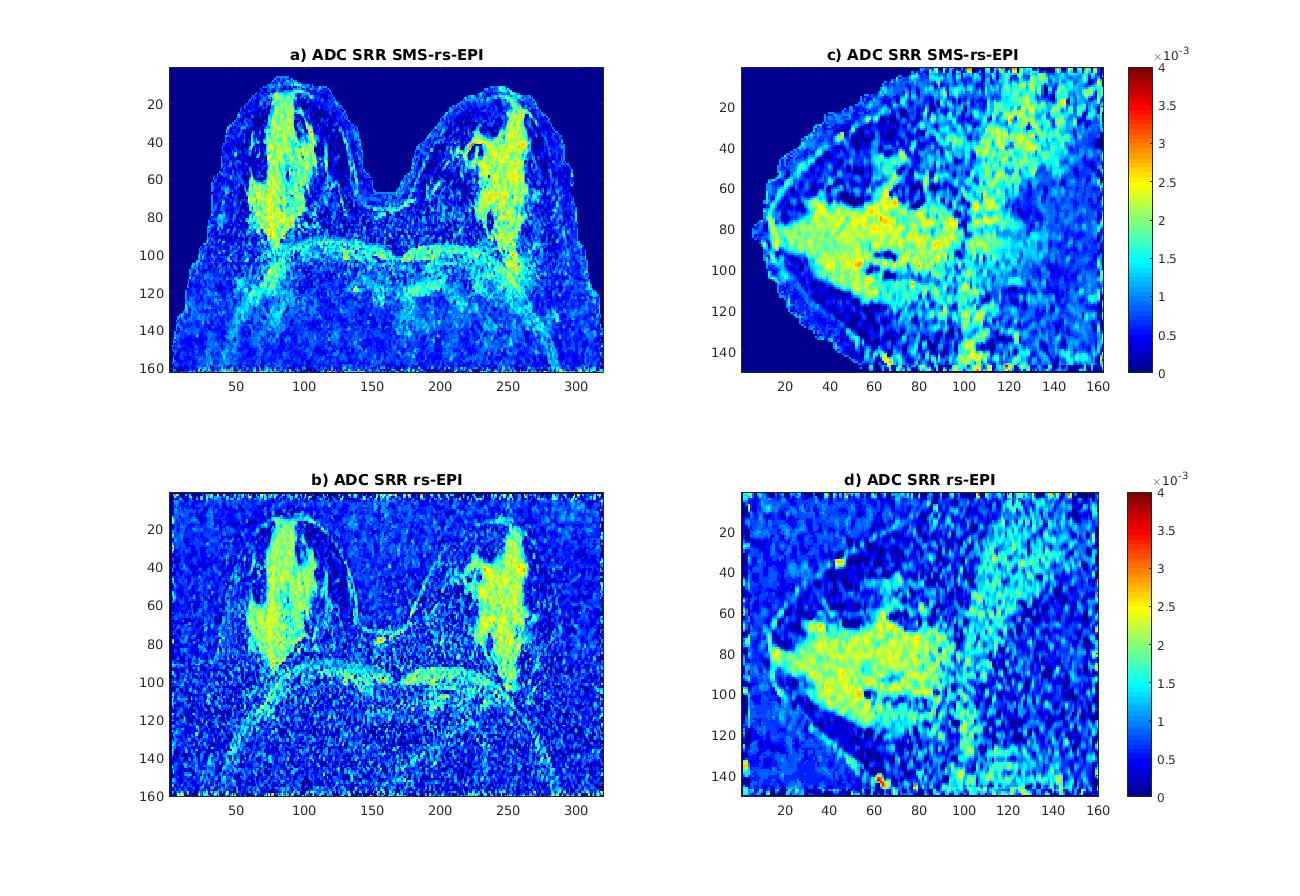
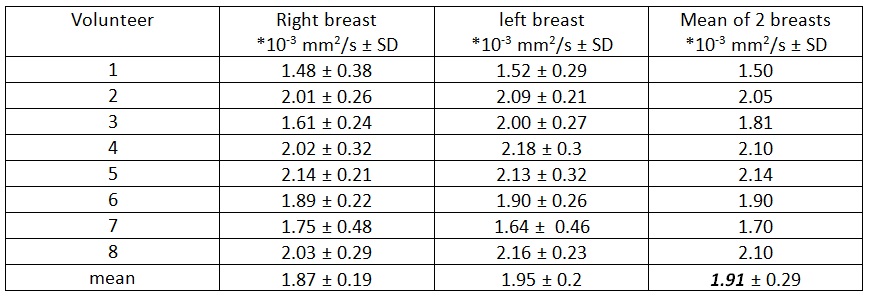
Figure 2 shows an example isotropic 1x1x1 mm3 ADC map in a subject, with/without SMS. Table 3 shows the mean ADC values (averaged over the eight subjects and the two breasts) which were 1.91 x10-3 mm2/s ± 0.29 with unaccelerated SRR. In the subject with/without SMS the ADC values were 2.05 and 2.1 *10-3 mm2/s.
Discussion and Conclusion
The results demonstrate the feasibility of HR DWI using the SRR. The use of SMS allows a significant reduction of the total scan time (below 10 min) with good preservation of SNR, spatial resolution and ADC values. Future work will be focused on applying the technique to patients to investigate the ability of the protocol to detect breast tumors. HR DWI could have a fundamental role in screening high-risk women. Besides, it might be used for predicting treatment outcome in breast cancer without the need for a contrast agent. It could also reduce the number of examinations using contrast agent injection.Acknowledgements
Grant funding: ANR-17-CE19-0022 (Bracoil project) and INCA, Plan Cancer 2014-19 (Screenbreast project). The authors also thank Khalid Ambarki (Siemens Healthineers, Saint-Denis, France) and Wei Liu (Siemens Healthineers, Shenzen, China) for providing the SMS-rs-EPI sequence prototype, and Institut de Cancérologie de Lorraine, INSERM, FEDER and Région Lorraine.
References
1. Kul S, Metin Y, Kul M, Metin N, Eyuboglu I, Ozdemir O. Assessment of breast mass morphology with diffusion-weighted MRI: Beyond apparent diffusion coefficient: Breast DWI for the Evaluation of Mass Morphology. J Magn Reson Imaging [Internet]. 2018 May 7 [cited 2018 May 15]; Available from: http://doi.wiley.com/10.1002/jmri.26175
2. Filli L, Ghafoor S, Kenkel D, Liu W, Weiland E, Andreisek G, et al. Simultaneous multi-slice readout-segmented echo planar imaging for accelerated diffusion-weighted imaging of the breast. Eur J Radiol. 2016 Jan;85(1):274–8.
3. Maya Delbany, Bustin A, POUJOL J, Thomassin-Naggara I, Felblinger J, Vuissoz P-A, et al. One-millimeter isotropic breast DWI: evaluation of a super-resolution strategy in terms of signal-to-noise ratio, sharpness and apparent diffusion coefficient. Magn Reson Med. In press;
4. Setsompop K, Gagoski BA, Polimeni JR, Witzel T, Wedeen VJ, Wald LL. Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty. Magn Reson Med. 2012 May 1;67(5):1210–24.
5. Reeder SB, Wintersperger BJ, Dietrich O, Lanz T, Greiser A, Reiser MF, et al. Practical approaches to the evaluation of signal-to-noise ratio performance with parallel imaging: Application with cardiac imaging and a 32-channel cardiac coil. Magn Reson Med. 2005 Sep;54(3):748–54.
Figures