1852
Initial evaluation of an automated acquisition workflow for multiparametric MR (spectroscopic) imaging of the prostate1Radiology and Nuclear Medicine, Radboud university medical center, Nijmegen, Netherlands, 2Application Development, Siemens Healthcare GmbH, Erlangen, Germany, 3Norwegian University of Science and Technology, Trondheim, Norway, 4St. Olavs Hospital, Trondheim University Hospital, Trondheim, Norway
Synopsis
Standardization of imaging and automated adjustment of MR parameters could homogenize and expedite multiparametric MRI of the prostate. If automated and robust, spectroscopic imaging (MRSI) could be a part of this protocol. In this dual-centre study, an automated workflow was validated by patient measurements at 3T MR systems and the robustness of the spectroscopic imaging approach was evaluated. Automation of the acquisition protocol of multiparametric MR imaging of the prostate needed only minor manual adjustments. On average, 84% of the MRSI voxels within the prostate passed our quality control, illustrating the current robustness of the automated semi-LASER MRSI technique.
Introduction
With the rapidly growing importance and use of multiparametric MRI (mpMRI) exams of the prostate in clinical practice, there is need for improved, faster and computer-aided data acquisition workflows. For MR spectroscopic imaging (MRSI), standardization and automation of acquisition parameters could expedite clinical application of this technique. For these purposes, the Prostate Dot engine is under development, which allows automated positioning of the MR measurements based on automatic segmentation of the prostate. The aim of this dual-centre study was to validate the automated workflow and to assess the robustness of the latest semi-LASER spectroscopic imaging and postprocessing approach1.Methods
Twenty consecutive patients with suspected prostate cancer, referred to clinical prebiopsy mpMRI, were scanned with the automated workflow prototype, consisting of a normal clinical protocol (T2 weighted TSE in 3 directions, DWI, T1 weighted DCE MRI) supplemented with a semi-LASER 1H MRSI sequence. The 3T MRI systems (MAGNETOM Prisma-fit2, n=17; MAGNETOM Skyra2, n=3) were used with a spine and body-array coil for signal reception.
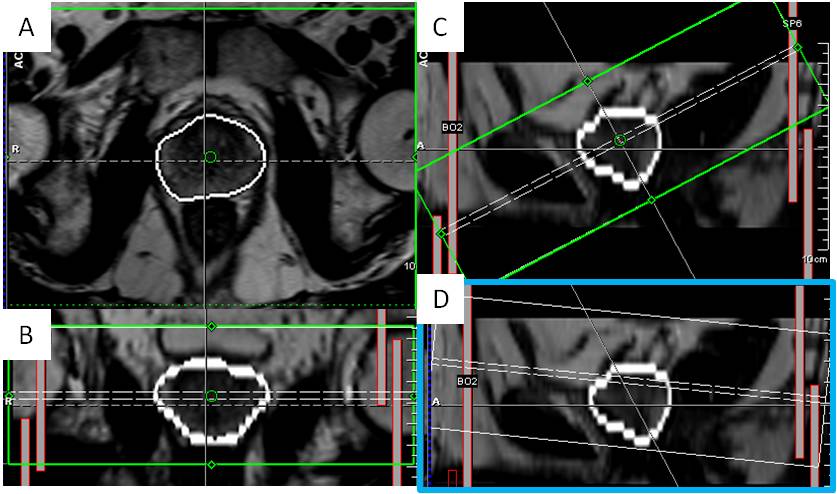
After an initial 35-second T2w-TSE scan the prostate segmentation algorithm was run together with the detection of bladder neck and exit point of the urethra as landmarks. Based on this segmentation, the acquisition protocols were automatically aligned parallel and perpendicular to the line between the two landmarks to cover the complete prostate gland. This automated workflow, so-called Prostate Dot engine2, was evaluated by visually assessing the performance and tracking manual labor. The focus is on segmentation of the prostate, axial slice angulation, positioning of spectroscopic volume of interest (VOI), and outer volume saturation (OVS) bands.
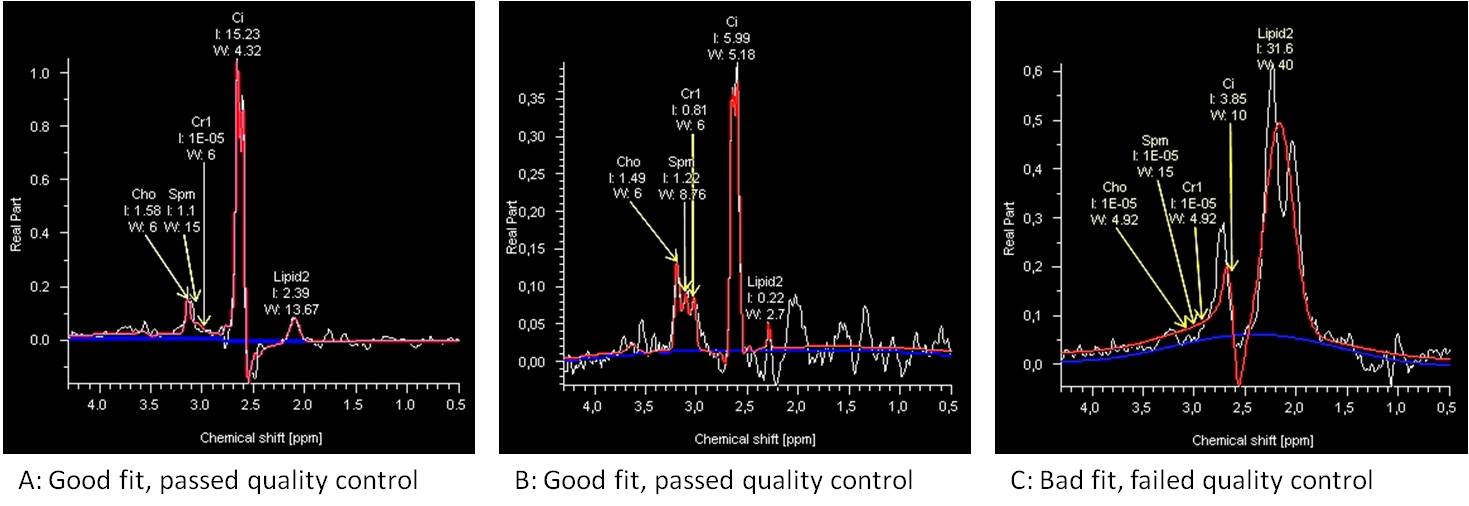
MRSI results (voxel size 7x7x7mm) were displayed in syngo.via2 and processed with a custom-made protocol fed with simulated metabolite model files for the specific timing of the semi-LASER pulse sequence (TE 88ms). Saturated voxels and voxels outside of the prostate were rejected and remaining voxels had to pass a quality control (QC). Conditions for QC focused on metabolite peak fit to noise ratio, lipid residual and citrate peak phase. The percentage of voxels within the prostate that produced high quality spectra was used as a measure for robustness of the semi-LASER MRSI pulse sequence combined with the automated positioning technique.
Results
The segmentation performed well in 15/20 patients on visual inspection and was used to estimate the necessary number of slices and slice-pack positioning to cover the prostate. In 5 patients parts of the peripheral zone of the prostate were overestimated, requiring some manual adjustments of the imaging slice packages and MRSI saturation slabs (one patient with brachytherapy seeds).
Within the automatic workflow, a small selection of parameters can easily be adapted. Due to the preference of our clinic to cover the prostate from base to apex, rather than perpendicular to the urethra as done by the automated workflow, the proposed angulation was changed manually for every patient (Fig.1). The adapted angulation is automatically copied to other axial acquisitions (DWI and DCE-MRI).
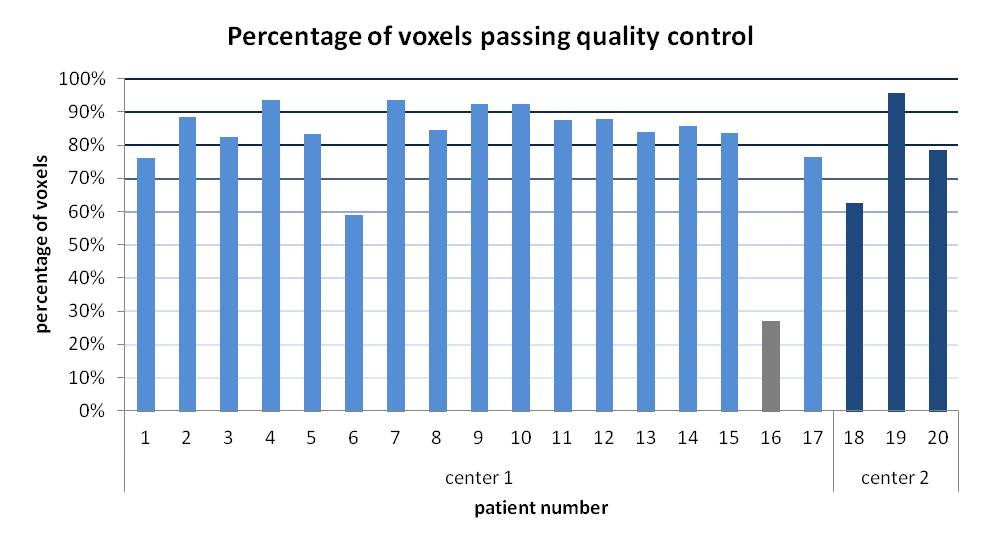
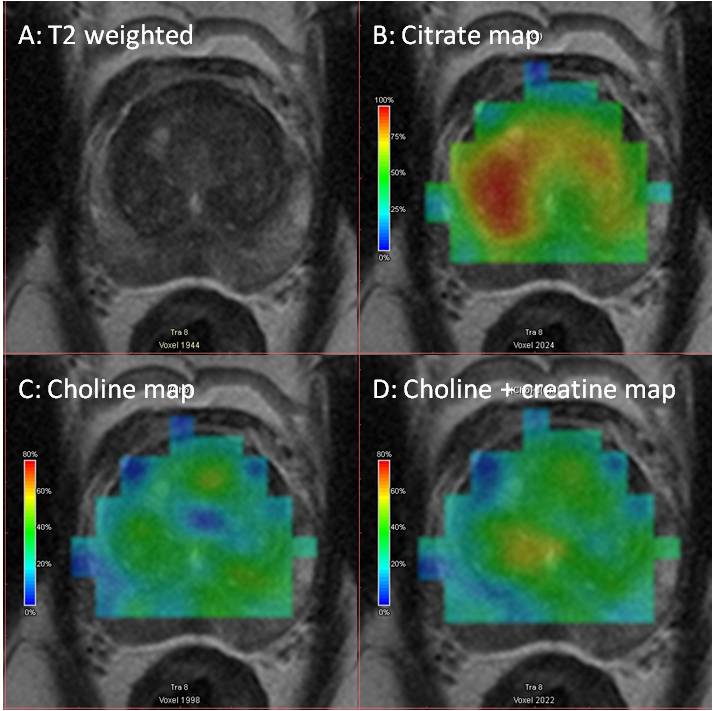
QC of the MRSI data was performed per voxel. 84% of all voxels was rated as good quality, with 17 out of 19 patients (excluding the brachytherapy patient) scoring above 75% of voxels within the prostate that passed QC (Fig.3). The high ratio of good quality spectra enabled visualization of the metabolite distributions across the prostate, shown in figure 4. As a measure of prostate size, the number of voxels within the prostate per patient could be used, which had a median value of 500 voxels (interquartile range 210) and showed no correlation with the percentage of voxels with good quality spectra (Pearson’s r=0.27, p>0.1).
Discussion
The automatic workflow enables mpMRI with little manual interaction. The automated placement of MRSI settings provides a good base and requires only small manual adjustments to result in robust MRSI, independent of prostate size.
The post-processing method for MRSI was efficient for displaying good quality spectra. Further improvements can be made to the QC method, e.g. by incorporating machine learning techniques3.
Once pathological data becomes available by follow-up of these patients, a quantitative assessment of metabolite ratios will give insight in the clinical value of this specific semi-LASER spectroscopic imaging approach.
Conclusion
In general, the automated workflow for mpMRI of the prostate at 3T is feasible with only minor manual adjustments. The automated set-up of spectroscopic imaging parameters (VOI, FOV and OVS bands) standardizes positioning and saves adjustment time, which could enable its usage for less experienced technicians. With an automated QC an average of 84% of voxels within the prostate is found of good quality, which highlights the current robustness of semi-LASER MRSI of the prostate.Acknowledgements
No acknowledgement found.References
1. Steinseifer, I.K., et al., Improved Volume Selective 1H MR Spectroscopic Imaging of the Prostate with Gradient Offset Independent Adiabaticity Pulses at 3 Tesla. Magnetic Resonance in Medicine, 2015. 74: p. 915–924.
2. Siemens Healthcare GmbH, Erlangen, Germany
3. Wright, A.J., et al., Quality control of prostate 1 H MRSI data. NMR in Biomedicine, 2013. 26(2): p. 193-203
Figures