1851
MRI of the prostate using a two-channel phased-array endorectal receive coil compared to phased array coil acquisition1Department of Radiology, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 2Translational and Molecular Imaging Institute, Icahn School of Medicine at Mount Sinai, New York, NY, United States, 3InVivo Corporation, Philips Healthcare, Gainesville, FL, United States, 4Department of Urology, Icahn School of Medicine at Mount Sinai, New York, NY, United States
Synopsis
In this study, 3T MRI of the prostate using a two-channel solid phased-array endorectal receive coil (ERC) (Sentinelle, InVivo Corporation, Philips Healthcare) combined with phased array coil (PAC) was compared to PAC only for image quality and lesion conspicuity on T2WI and DWI. Improved image quality was found for T2WI and high b-value DWI and improved lesion contrast using ERC-PAC, while there was no difference in lesion conspicuity. These preliminary results show that the use of ERC-PAC improves prostate MRI image quality, without necessarily impacting lesion detection.
Purpose
Multiparametric MRI (mpMRI) of the prostate, using a combination of T2WI, DWI and DCE-MRI, is highly valuable for prostate cancer (PCa) detection and characterization (1,2). Prostate MRI using 3T MR and a phased array body coil (PAC) is the current practice standard (3,4). Mixed results have been shown comparing image quality and lesion detection when comparing PAC to balloon-inflatable endorectal coil using 3.0T (5-8). A new rigid two-channel receive endorectal coil (ERC) has shown improved SNR and image quality on T2W compared to the balloon-inflatable ERC at 1.5T, with less prostate deformation (9,10). Disposable rigid ERC devices have been developed with equivalent coil profiles compared to the reusable device. The use of the rigid ERC combined with external PAC and parallel imaging provides further opportunities to improve SNR, potentially translating to improved image quality and lesion detection. The goal of this study was to intra-individually compare image quality and lesion conspicuity of 3T mpMRI using a PAC compared to a combined rigid ERC and PAC (ERC-PAC), and to assess patient comfort.Methods
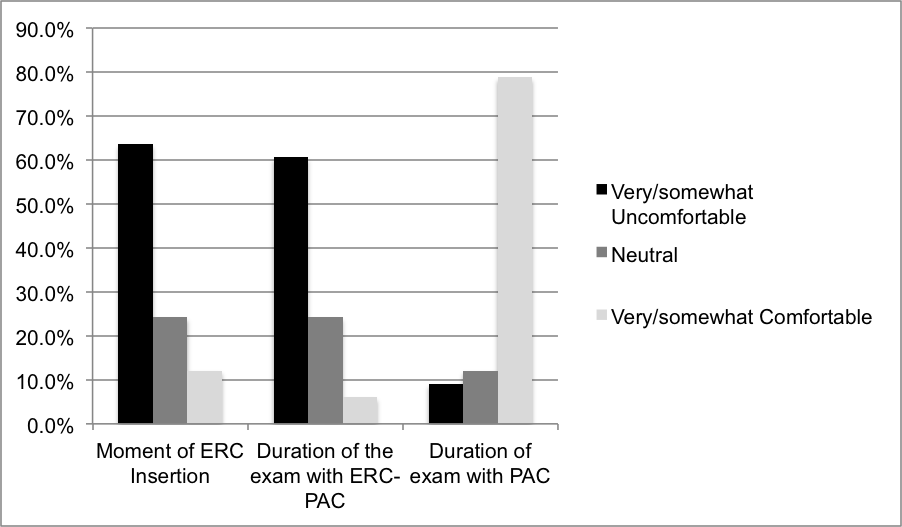
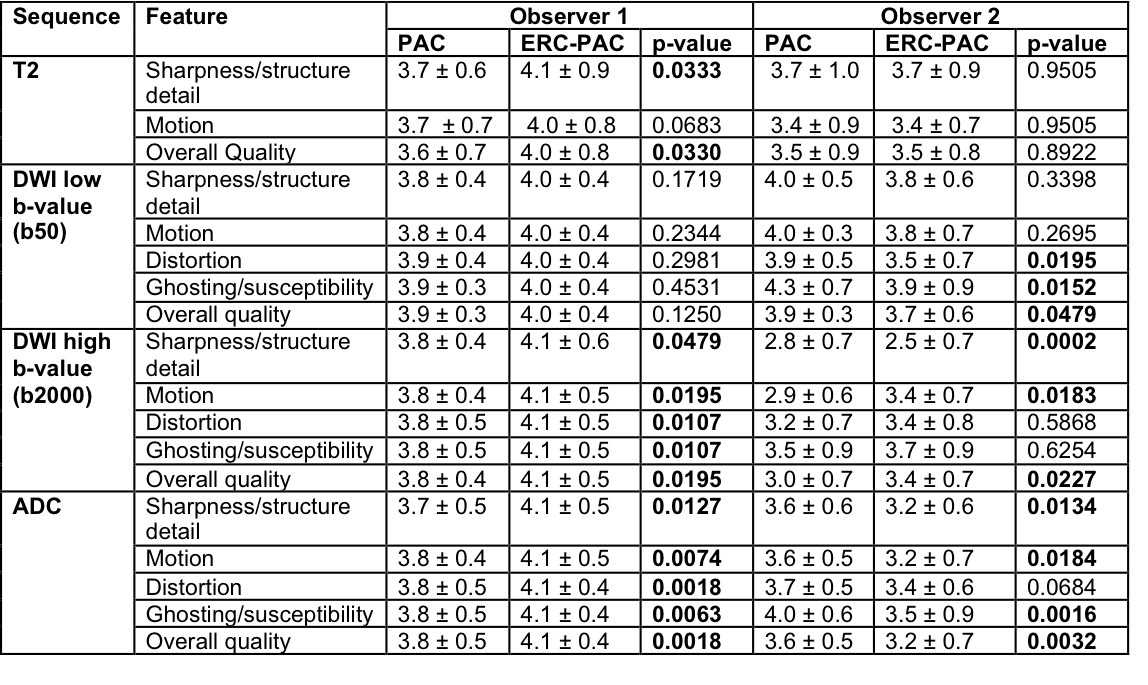
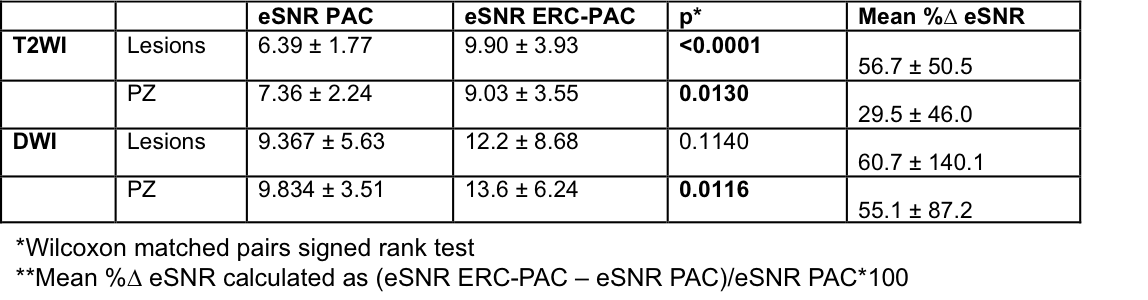
33 men (mean age 65.3y, mean PSA 9.9ng/mL, mean PSA density 0.15) with suspected (n=14) or biopsy-proven PCa (n=19) were prospectively enrolled in this IRB-approved study from 2/2017-8/2018. Inclusion criteria included men with biopsy-proven PCa, elevated PSA or positive physical exam. Men previously treated for PCa were excluded. All patients underwent prostate 3T mpMRI (Skyra, Siemens) using a rigid phased-array ERC (Sentinelle, InVivo Corporation, Philips Healthcare) and PAC only (18-elements). Rigid ERC devices used included a reusable coil (n=20) or disposable coil (n=13). Patients were randomized to one of two protocols: Protocol A (Axial T2 and DWI using ERC-PAC; followed by multiplanar T2, DWI and DCE-MRI using PAC; n=18) or Protocol B (Axial T2 and DWI with PAC; followed by multiplanar T2, DWI and DCE-MRI using ERC-PAC; n=15). Sequence parameters were identical for both PAC and ERC-PAC acquisitions. Two observers independently evaluated DWI and T2 using PAC and ERC-PAC in a random order for image quality (sharpness, motion, distortion, ghosting, coil artifacts, overall quality) on a 5-point scale (1: non-diagnostic; 5: excellent), lesion detection (PIRADS v2) and conspicuity on a 5-point scale (1: not visualized; 5: excellent conspicuity). ROIs were placed on prostate lesions and PZ to measure estimated SNR [eSNR as mean signal intensity (SI)/SD_SI] in the ROI on T2 and b2000 DWI images. Lesion-to-PZ contrast ratios (CR) were calculated for T2 and DWI for both acquisitions [CR=(SI_lesion-SI_PZ)/(SI_lesion+SI_PZ)]. Patient comfort was assessed on a questionnaire at the time of ERC insertion, during the exam for ERC-PAC and PAC (1, very uncomfortable; 5, very comfortable) and whether he would prefer an MRI exam with the ERC-PAC if superior diagnostic accuracy were found. Data were compared for sequences between acquisitions using the Wilcoxon matched pairs signed-rank test. Agreement for PIRADS classification was assessed.Results
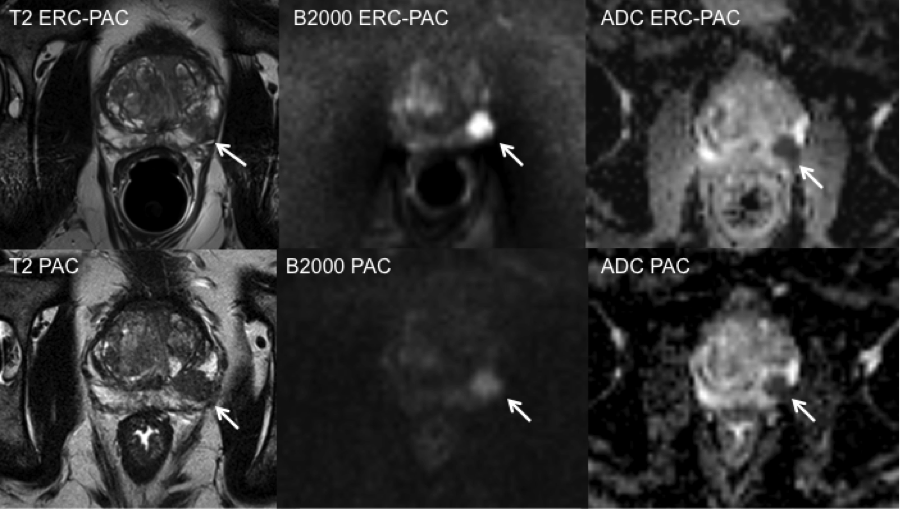
23 prostate lesions (including 20 biopsy-proven PCa) were identified in 23/33 men. Representative T2, DWI and ADC maps from ERC-PAC and PAC are shown in Fig. 1. Higher image quality scores for ERC-PAC were observed for T2 (significant for 1 observer, p=0.0330) and high b-value DWI (significant for both observers p=0.0195-0.0227), with mixed results for low b-value DWI and ADC maps (Table 1). ERC-related artifacts were worse on T2 compared to DWI and ADC (significant for 1 observer, p-values <0.0003). There was fair-to-very good agreement between ERC-PAC and PAC acquisitions for PIRADS categorization for T2/DWI/Overall (k=0.36/0.61/0.37 and k=0.83/0.72/0.71 for observers 1 and 2).There was no difference in lesion conspicuity for ERC-PAC or PAC for T2 and DWI(both observers, all p-values >0.1719). There was higher eSNR for sequences performed using ERC-PAC, except for lesions (Table 2). Higher lesion-PZ CR was found for DWI using ERC-PAC (Table 3).Results from the patient questionnaire are shown in Fig 2. 97% (32/33) of patients reported definitely or probably choosing to have an exam with ERC-PAC if superior diagnostic accuracy is shown.Discussion and Conclusions
We found overall improved image quality on T2 and high b-value DWI for exams performed using a rigid ERC-PAC compared to PAC alone with mixed results for low b-value DWI and ADC. There was equivalent lesion classification and conspicuity for both acquisitions on both T2 and DWI. As expected, higher eSNR on T2WI and DWI and higher lesion-PZ CR on DWI using ERC-PAC were observed. The majority of patients reported discomfort with the use of the ERC, although nearly all reported preferring the use of an ERC should improved PCa detection rates be achieved. Further analysis is ongoing to assess the diagnostic performance of MRI using a rigid ERC-PAC versus PAC for PCa detection and staging.Acknowledgements
No acknowledgement found.References
1. Hegde JV, Mulkern RV, Panych LP, et al. Multiparametric MRI of prostate cancer: an update on state-of-the-art techniques and their performance in detecting and localizing prostate cancer. Journal of magnetic resonance imaging : JMRI 2013;37(5):1035-1054.
2. Donati OF, Afaq A, Vargas HA, et al. Prostate MRI: evaluating tumor volume and apparent diffusion coefficient as surrogate biomarkers for predicting tumor Gleason score. Clinical cancer research : an official journal of the American Association for Cancer Research 2014;20(14):3705-3711.
3. Shah ZK, Elias SN, Abaza R, et al. Performance comparison of 1.5-T endorectal coil MRI with 3.0-T nonendorectal coil MRI in patients with prostate cancer. Academic radiology 2015;22(4):467-474.
4. Leake JL, Hardman R, Ojili V, et al. Prostate MRI: access to and current practice of prostate MRI in the United States. Journal of the American College of Radiology : JACR 2014;11(2):156-160.
5. Turkbey B, Merino MJ, Gallardo EC, et al. Comparison of endorectal coil and nonendorectal coil T2W and diffusion-weighted MRI at 3 Tesla for localizing prostate cancer: correlation with whole-mount histopathology. Journal of magnetic resonance imaging : JMRI 2014;39(6):1443-1448.
6. Heijmink SW, Futterer JJ, Hambrock T, et al. Prostate cancer: body-array versus endorectal coil MR imaging at 3 T--comparison of image quality, localization, and staging performance. Radiology 2007;244(1):184-195.
7. Barth BK, Cornelius A, Nanz D, Eberli D, Donati OF. Comparison of image quality and patient discomfort in prostate MRI: pelvic phased array coil vs. endorectal coil. Abdom Radiol (NY) 2016;41(11):2218-2226.
8. Baur AD, Daqqaq T, Wagner M, et al. T2- and diffusion-weighted magnetic resonance imaging at 3T for the detection of prostate cancer with and without endorectal coil: An intraindividual comparison of image quality and diagnostic performance. European journal of radiology 2016;85(6):1075-1084.
9. Haider MA, Krieger A, Elliott C, Da Rosa MR, Milot L. Prostate imaging: evaluation of a reusable two-channel endorectal receiver coil for MR imaging at 1.5 T. Radiology 2014;270(2):556-565.
10. Martin GV, Kudchadker RJ, Bruno TL, Frank SJ, Wang J. Comparison of prostate distortion by inflatable and rigid endorectal MRI coils in permanent prostate brachytherapy imaging. Brachytherapy 2018;17(2):298-305.
Figures