1850
Prostate cancers invisible on multi-parametric MRI: Pathologic feature in correlation with whole mount prostatectomy1Department Of Radiology, University of Chicago, Chicago, IL, United States, 2Department Of Pathology, University of Chicago, Chicago, IL, United States
Synopsis
This study investigates why some prostate cancers are not identified on mpMRI using ground truth reference from whole mount prostatectomy specimens. Unidentified cancers tend to exhibit lower Gleason grade and pathologic stage, smaller size, lower density of glands compared to surrounding tissue (sparse cancer lesions) and have different tissue composition, specifically higher lumen (associated with high ADC and T2) and lower epithelium (associated with low ADC and T2) compared to cancer lesions identified on MRI.
Introduction
Multiparametric MRI (mpMRI) is increasingly used for prostate cancer diagnosis and guiding biopsies. While mpMRI is very good at detecting cancers, still 15-30% of clinically significant cancers can be missed even by expert radiologists (1-3). While some of these studies investigated the characteristics of detected and missed cancers, we still do not have a clear understanding of why cancers are missed by mpMRI. Therefore, this study aims to investigate why some prostate cancers are not identified on mpMRI using ground truth reference from whole mount prostatectomy specimens.Methods
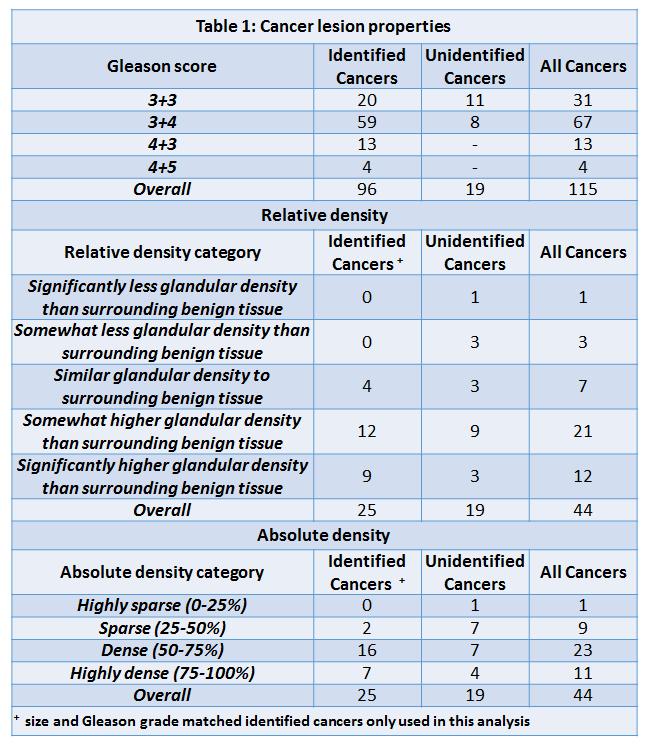
This IRB approved study involved retrospective analysis of prospectively acquired data. Patients (n=61) with biopsy confirmed prostate cancer (PCa) underwent preoperative 3T prostate mpMRI prior to undergoing radical prostatectomy. H&E stained whole mount prostatectomy specimens were prepared and cancers were outlined. MRI and histology sections were matched by an experienced radiologist (15 years’ experience). The lesion that were visible on MRI prospectively (blinded to pathology results) or retrospectively identified after correlating with histology were considered “identified cancers”. Lesions that could not be identified on mpMRI even after rad-path correlation were considered “unidentified cancers”. Quantitative MR parameters: ADC, T2 value and DCE-MRI parameters were calculated for representative ROIs. Two expert pathologists working in consensus marked the Gleason score, pathologic stage and size (dimension at section of largest extent) for all cancers. We further investigated all cancers that were undetected along with size and grade (Gleason 3+3 and 3+4) matched identified cancer. The relative density (scale 1-5, with 5 being highly dense compared to surrounding tissue) and absolute density scale (1-4, with 4 being highly dense cancer) of cancer glands was determined visually. Quantitative histology was performed to calculate fractional volumes of tissue components (stroma, epithelium and lumen) using Image Pro Premier on the basis of color, intensity, morphology and background with the “Smart Segment” tool similar to a previous study (4). Statistical tests: t-test (parametric) or Mann-Whitney U test (non-parametric) were performed to determine whether any significant difference between identified and unidentified cancers.Results
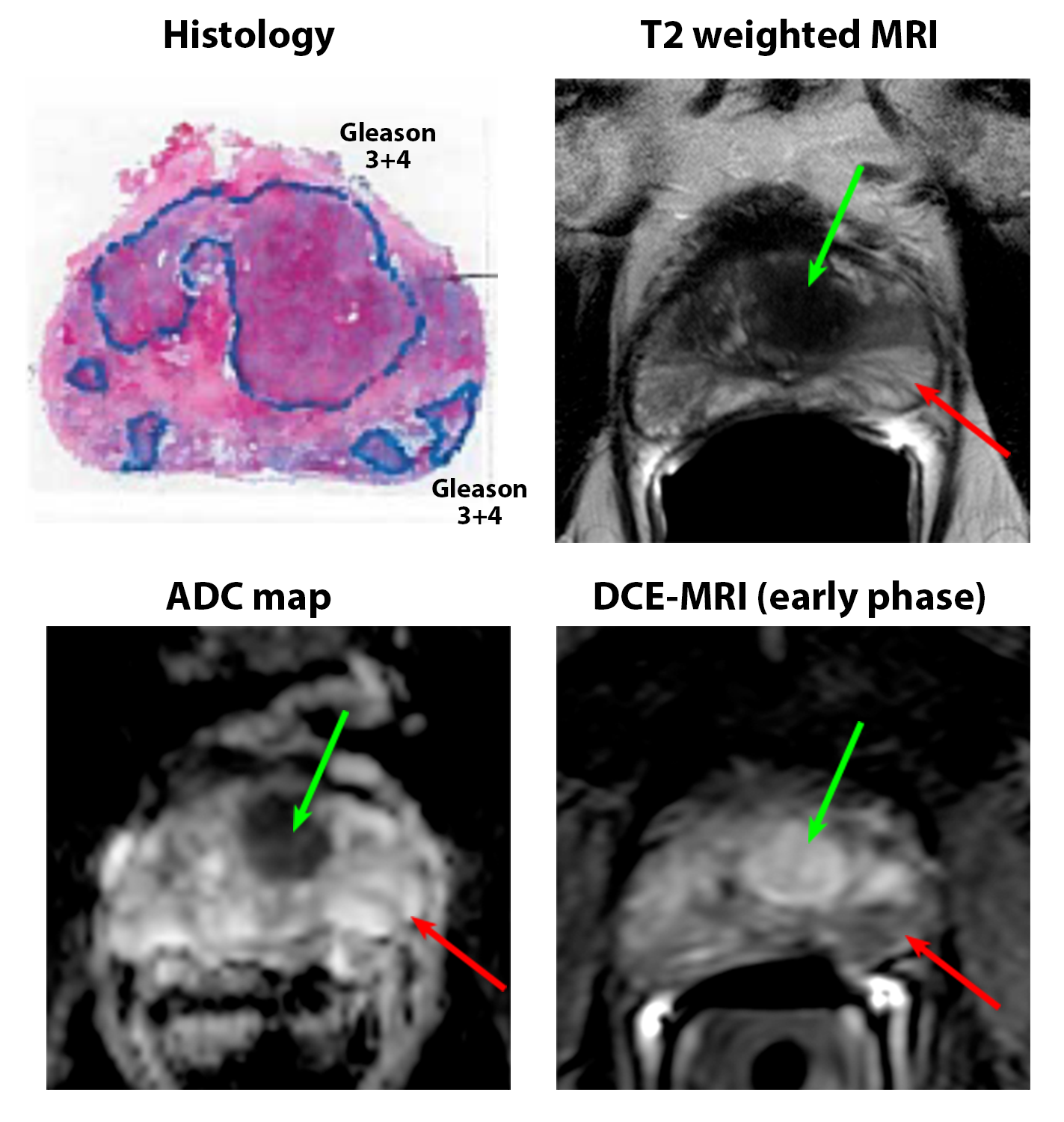
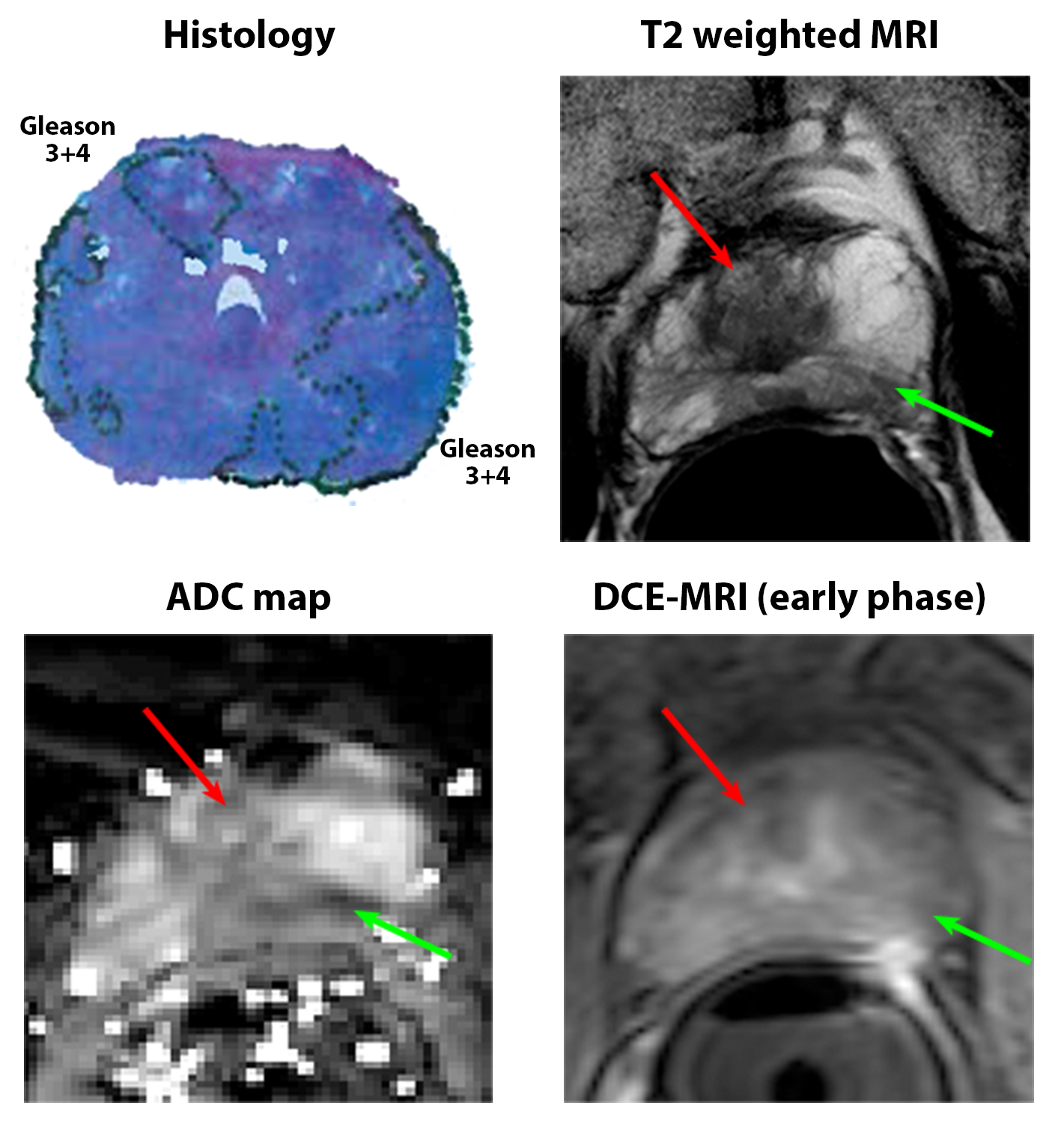
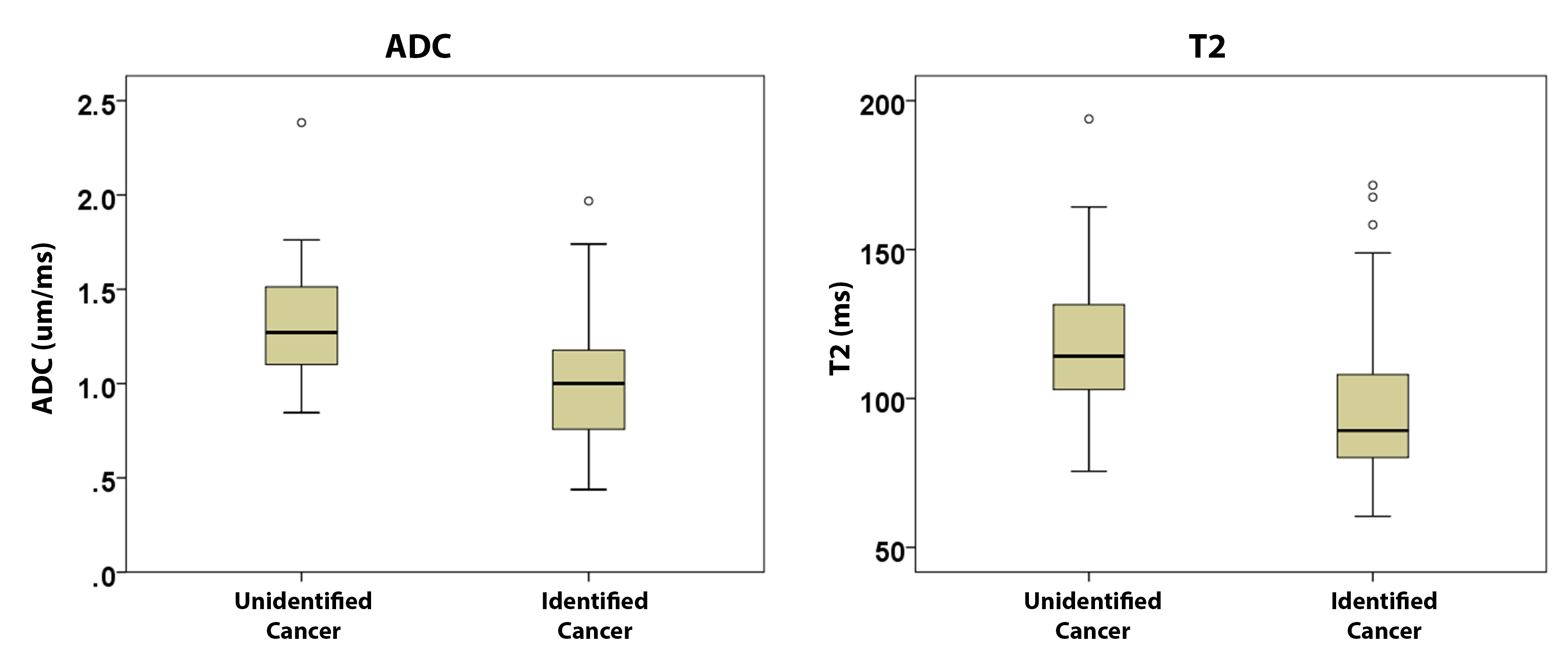
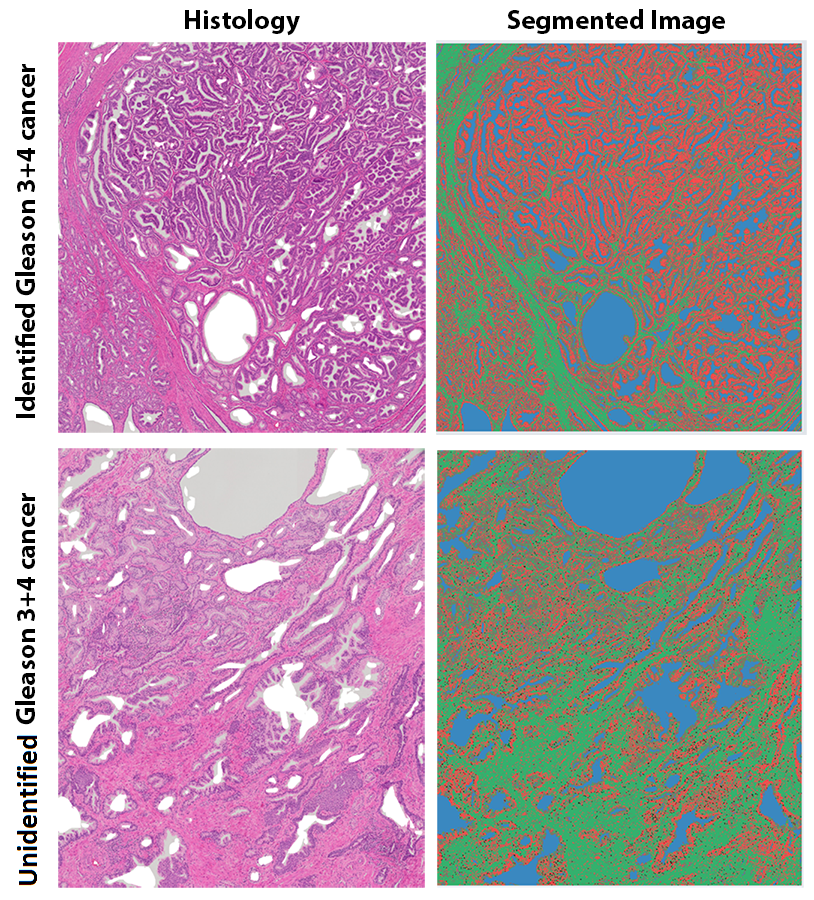
Representative images of identified and undefined cancers are shown in Figures 1 and 2. Only 19 of 115 confirmed cancerous lesions were unidentified on MRI. Unidentified cancers (1.4±1.0cm × 0.7±0.4cm) were significantly smaller in size than identified cancers (2.1±1.2cm × 1.0±0.5cm). Unidentified cancers were predominantly low grade (11 Gleason 3+3, 8 Gleason 3+4) and stage (all 19 were stage T2) compared to identified cancer (Grade: 20 Gleason 3+3, 59 Gleason 3+4, 13 Gleason 4+3, 4 Gleason 4+5; Stage: 68 Stage T2, 27 Stage T3). Unidentified cancer had significantly (p<0.05) higher ADC (1.34±0.38 vs 1.02±0.30 µm2/ms) and T2 (120.0±31.1 vs 97.1±25.1ms) compared to cancers visible on MRI, but DCE-MRI parameters were not significantly different (Fig 3).
For size and grade matched cancers, the relative density and absolute density of cancer glands was significantly (p=0.04) higher in cancers identified on MRI compared to the unidentified cancers (see Table 1). However, the percentage of Gleason 4 component in Gleason 3+4 lesions is only nominally (p=0.15) higher in identified cancers (20±12%) compared to unidentified cancers (15±8%). Preliminary investigation into the tissue composition of these cancers showed unidentified cancers had lower epithelium volume 28.6 vs 40.9% and higher lumen volume 23.5 vs 16.3% compared to unidentified cancers (Fig 4).
Some other observations by pathologists possibly explaining why some cancers were not identified were: adjacent cystic changes (n=2), small cancer focus (n=2), cancers being interspersed between atrophic glands (n=2) or benign glands (n=4), and surrounding dense glands (n=1).
Discussion
The unidentified cancers are smaller in size and have lower Gleason grade, which is in agreement with a previous study (5). Unidentified cancers also exhibit lower pathologic stage. When lesion size and grade of cancer was consistent, the relative density and absolute density of cancer glands was higher in identified cancers compared to the unidentified cancers (6). Importantly, tissue composition differences, specifically higher lumen (associated with high ADC and T2) and lower epithelium (associated with low ADC and T2) in unidentified cancers may explain why these lesions were missed on MRI. Comparing tissue composition to previous literature (4,7), unidentified cancers were found to have tissue composition similar to benign prostatic tissue and therefore appear similar to surrounding benign tissue and remain undetected on mpMRI.Conclusion
Prostate cancer lesions undetected on MRI tend to have lower glandular density and have similar tissue composition to benign tissue, along with being smaller in size and have lower Gleason grade compared to detected lesions.Acknowledgements
No acknowledgement found.References
1. Borofsky S, George AK, Gaur S, Bernardo M, Greer MD, Mertan FV, Taffel M, Moreno V, Merino MJ, Wood BJ, Pinto PA, Choyke PL, Turkbey B. What Are We Missing? False-Negative Cancers at Multiparametric MR Imaging of the Prostate. Radiology 2018;286(1):186-195.
2. Fütterer JJ, Briganti A, De Visschere P, Emberton M, Giannarini G, Kirkham A, Taneja SS, Thoeny H, Villeirs G, Villers A. Can Clinically Significant Prostate Cancer Be Detected with Multiparametric Magnetic Resonance Imaging? A Systematic Review of the Literature. European Urology 2015;68(6):1045-1053.
3. Schouten MG, van der Leest M, Pokorny M, Hoogenboom M, Barentsz JO, Thompson LC, Futterer JJ. Why and Where do We Miss Significant Prostate Cancer with Multi-parametric Magnetic Resonance Imaging followed by Magnetic Resonance-guided and Transrectal Ultrasound-guided Biopsy in Biopsy-naive Men? Eur Urol 2017;71(6):896-903.
4. Chatterjee A, Watson G, Myint E, Sved P, McEntee M, Bourne R. Changes in Epithelium, Stroma, and Lumen Space Correlate More Strongly with Gleason Pattern and Are Stronger Predictors of Prostate ADC Changes than Cellularity Metrics. Radiology 2015;277(3):751-762.
5. Tan N, Margolis DJ, Lu DY, King KG, Huang J, Reiter RE, Raman SS. Characteristics of Detected and Missed Prostate Cancer Foci on 3-T Multiparametric MRI Using an Endorectal Coil Correlated With Whole-Mount Thin-Section Histopathology. AJR Am J Roentgenol 2015;205(1):13285.
6. Langer DL, van der Kwast TH, Evans AJ, Sun L, Yaffe MJ, Trachtenberg J, Haider MA. Intermixed normal tissue within prostate cancer: effect on MR imaging measurements of apparent diffusion coefficient and T2--sparse versus dense cancers. Radiology 2008;249(3):900-908.
7. Langer DL, van der Kwast TH, Evans AJ, Plotkin A, Trachtenberg J, Wilson BC, Haider MA. Prostate tissue composition and MR measurements: investigating the relationships between ADC, T2, K(trans), v(e), and corresponding histologic features. Radiology 2010;255(2):485-494.
Figures