1849
Towards a clinic-radiologic-biopsy based predictive model for the detection of pelvic lymph node invasion in patients with prostate cancer before surgeryying hou1
1radiology, the First Affiliated Hospital with Nanjing Medical University, nan jing, China
Synopsis
Pelvic lymph node invasion in patients with prostate cancer is associated with different treatment selection and planning while there is no clear consensus on nomograms that can be clinically available for prediction of lymph node invasion. Our predictive model, based on preoperative clinical characteristics, MR image features and biopsy findings of 248 consecutive patients, was trained with a support vector machine and compared to a logistic regression analysis, allowing for improved differentiation in assessing the risk of lymph node invasion. Use of this machine-learning-based predictive tool potentially connect to better selection of optimal type of treatment and long-term excellent prognosis.
Introduction
Pre-treatment identification of prostate cancer(PCa) spread to the lymph nodes (LNs) is a critical indicator for patient counseling, clinical staging and appropriate treatment selection and planning(1-4). Although several nomograms have been developed to assess the possibility of lymph node invasion(LNI)(5-14), there is still no clear consensus on nomograms that can be clinically available for prediction of LNI in patients with PCa(15, 16).Our study expected to establish a predictive model based on preoperative clinical characteristics, MRI image features and biopsy findings to predict LNI prospectively, increasing diagnosis accuracy.Materials and methods
A total of 248 consecutive patients (mean age, 69.9 ± 0.4 years; range, 47-86 years) were identified and comprised the primary cohort according to the patient recruitment pathway as well as the inclusion and exclusion criteria listed in Fig. 1. Image analysis was performed by two independent readers blinded to any clinical information and histopathologic examination served as the standard of reference. In all, 4 clinical characteristics, 10 MRI image features and 4 biopsy findings were recorded, which were listed in Table 1. Predictive models were developed from these features to assess the prevalence of LNI, using a logistic regression (LR) and support vector machine (SVM) analysis, respectively.Results
Total 59/248 (23.8%) LNI patients were identified at surgery. RFE-SVM analysis selected total 6 most important features which produced largest area under the receiver operating curve (AUC) and smallest bias over the bootstrapping validation (Fig. 2). In LR model, 4 independent features were determined at significant level with the multivariate regression analysis. The coefficient of features selected and adjusted odds ratio (OR) estimated by LR analysis were summarized in Table 2. The receiver operating curve (ROC) analysis shows that SVM yielded higher AUC (0.94, 95 confidence intervals [CI], 0.92-0.95 vs 0.90, 95% CIs, 0.88-0.91; p < 0.001) than LR analysis (Fig. 3). Conventional radiologic-lymph node (LN) report had high specificity (97.9%) and low sensitivity (39.0%) for diagnosis of LNI. In radiologic LN-negative subgroup, SVM and LR model identified 33/36 (91.7%) and 27/36 (75%) additional positive cases, respectively. SVM and LR model had similar sensitivity (95.7% vs 100%) and same specificity (25% vs 25%) in mr-LN+ subgroup. In mr-LN- subgroup, SVM model resulted in higher sensitivity (91.7% vs 75%) and higher specificity (88.1% vs 80.0%) than LR model (Table 3).Discussion
In this study, we established a clinic-radiologic-biopsy based predictive model to better diagnostic performance in LNI. The results reveal that our two predictive models, especially the SVM one, play a promising performance in improving diagnostic accuracy. For component factors analysis, mr- seminal vesicle invasion (SVI), Apparent diffusion coefficient(ADC), D-max and number of positive cores had been proved to be independent risk factors for predicting histopathologic LNI in our both two models, while serum prostate specific antigen (PSA) level and mr- extracapsular extension (ECE) were also significant in SVM one. To our knowledge, mr-SVI, D-max and mr-ECE signified greater odds of cancer aggressiveness and malignant potential (17, 18), while PSA and number of positive cores rather suggest the probability of pathologic state. For ADC evaluation, quantitative ADC is a reliable surrogate of cancerous GS, indicating biological properties(19). Comparing our two diagnostic models, SVM model is superior to LR model with an AUC of 0.94 vs 0.90. The excellent performance of SVM approach can be attributed to its optimal generalization ability, which can progressively learn from misclassified examples and automatically remove the false positives via examination of the distance in the Hilbert space to avoid over-fitting(20, 21). On the contrast, factors are independently associated with LNI on LR analysis. Similarly making full use of preoperative variables, our study was in line with those published studies(14, 22, 23). In the study of Brembilla et al.(22), combining MR-stage and clinical characteristics, the model yielded the highest accuracy (AUC, 0.956). In another study of Wang et at.(14), MR variables merged with a Partin nomogram significantly improved predictive performance. Compared with these models, we acceded more variables such as mr-ECE, mr-SVI and PI-RADS scores, all of which are easy-to-obtain by radiologists in their routine assignment for prostatic MRI. And all the quantitative variables were transformed to categorical data to cut down the influence of extremum.Conclusion
The designed predictive model is better than conventional radiologic reporting way for predicting LNI in patients with PCa. The utility of this approach can be viewed in terms of enhancing both the diagnosis and treatment processes.Acknowledgements
No acknowledgement found.References
1. Mottet N, Bellmunt J, Bolla M, Briers E, Cumberbatch MG, De Santis M, et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. European urology. 2017;71:618-29. 2. Mohler J, Bahnson RR, Boston B, Busby JE, D'Amico A, Eastham JA, et al. NCCN clinical practice guidelines in oncology: prostate cancer. Journal of the National Comprehensive Cancer Network : JNCCN. 2010;8:162-200. 3. Gakis G, Boorjian SA, Briganti A, Joniau S, Karazanashvili G, Karnes RJ, et al. The role of radical prostatectomy and lymph node dissection in lymph node-positive prostate cancer: a systematic review of the literature. European urology. 2014;66:191-9. 4. Allaf ME, Partin AW, Carter HB. The importance of pelvic lymph node dissection in men with clinically localized prostate cancer. Reviews in urology. 2006;8:112-9. 5. Partin AW, Kattan MW, Subong EN, Walsh PC, Wojno KJ, Oesterling JE, et al. Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer. A multi-institutional update. Jama. 1997;277:1445-51. 6. Briganti A, Gallina A, Suardi N, Chun FK, Walz J, Heuer R, et al. A nomogram is more accurate than a regression tree in predicting lymph node invasion in prostate cancer. BJU international. 2008;101:556-60. 7. Briganti A, Larcher A, Abdollah F, Capitanio U, Gallina A, Suardi N, et al. Updated nomogram predicting lymph node invasion in patients with prostate cancer undergoing extended pelvic lymph node dissection: the essential importance of percentage of positive cores. European urology. 2012;61:480-7. 8. Jung SI, Donati OF, Vargas HA, Goldman D, Hricak H, Akin O. Transition zone prostate cancer: incremental value of diffusion-weighted endorectal MR imaging in tumor detection and assessment of aggressiveness. Radiology. 2013;269:493-503. 9. Vargas HA, Akin O, Franiel T, Mazaheri Y, Zheng J, Moskowitz C, et al. Diffusion-weighted endorectal MR imaging at 3 T for prostate cancer: tumor detection and assessment of aggressiveness. Radiology. 2011;259:775-84. 10. Yakar D, Debats OA, Bomers JG, Schouten MG, Vos PC, van Lin E, et al. Predictive value of MRI in the localization, staging, volume estimation, assessment of aggressiveness, and guidance of radiotherapy and biopsies in prostate cancer. Journal of magnetic resonance imaging : JMRI. 2012;35:20-31. 11. Studer UE, Scherz S, Scheidegger J, Kraft R, Sonntag R, Ackermann D, et al. Enlargement of regional lymph nodes in renal cell carcinoma is often not due to metastases. The Journal of urology. 1990;144:243-5. 12. Woo S, Suh CH, Kim SY, Cho JY, Kim SH. The Diagnostic Performance of MRI for Detection of Lymph Node Metastasis in Bladder and Prostate Cancer: An Updated Systematic Review and Diagnostic Meta-Analysis. AJR American journal of roentgenology. 2018;210:W95-w109. 13. Porpiglia F, Manfredi M, Mele F, Bertolo R. Indication to pelvic lymph nodes dissection for prostate cancer: the role of multiparametric magnetic resonance imaging when the risk of lymph nodes invasion according to Briganti updated nomogram is <5. 2018;21:85-91. 14. Wang L, Hricak H, Kattan MW, Schwartz LH, Eberhardt SC, Chen HN, et al. Combined endorectal and phased-array MRI in the prediction of pelvic lymph node metastasis in prostate cancer. AJR American journal of roentgenology. 2006;186:743-8. 15. Barentsz JO, Thoeny HC. Prostate cancer: Can imaging accurately diagnose lymph node involvement? Nature reviews Urology. 2015;12:313-5. 16. Sartor O, Eisenberger M, Kattan MW, Tombal B, Lecouvet F. Unmet needs in the prediction and detection of metastases in prostate cancer. The oncologist. 2013;18:549-57. 17. Masterson TA, Pettus JA, Middleton RG, Stephenson RA. Isolated seminal vesicle invasion imparts better outcomes after radical retropubic prostatectomy for clinically localized prostate cancer: prognostic stratification of pt3b disease by nodal and margin status. Urology. 2005;66:152-5. 18. McNeal JE, Villers AA, Redwine EA, Freiha FS, Stamey TA. Histologic differentiation, cancer volume, and pelvic lymph node metastasis in adenocarcinoma of the prostate. Cancer. 1990;66:1225-33. 19. Wu CJ, Wang Q, Li H, Wang XN, Liu XS, Shi HB, et al. DWI-associated entire-tumor histogram analysis for the differentiation of low-grade prostate cancer from intermediate-high-grade prostate cancer. Abdominal imaging. 2015;40:3214-21. 20. Lee HJ, Hwang SI, Han SM, Park SH, Kim SH, Cho JY, et al. Image-based clinical decision support for transrectal ultrasound in the diagnosis of prostate cancer: comparison of multiple logistic regression, artificial neural network, and support vector machine. European radiology. 2010;20:1476-84. 21. Gaspar P, Carbonell J, Oliveira JL. On the parameter optimization of Support Vector Machines for binary classification. Journal of integrative bioinformatics. 2012;9:201. 22. Brembilla G, Dell'Oglio P, Stabile A, Ambrosi A, Cristel G, Brunetti L, et al. Preoperative multiparametric MRI of the prostate for the prediction of lymph node metastases in prostate cancer patients treated with extended pelvic lymph node dissection. European radiology. 2018;28:1969-76. 23. Park SY, Oh YT, Jung DC, Cho NH, Choi YD, Rha KH. Prediction of Micrometastasis (< 1 cm) to Pelvic Lymph Nodes in Prostate Cancer: Role of Preoperative MRI. AJR American journal of roentgenology. 2015;205:W328-34.Figures
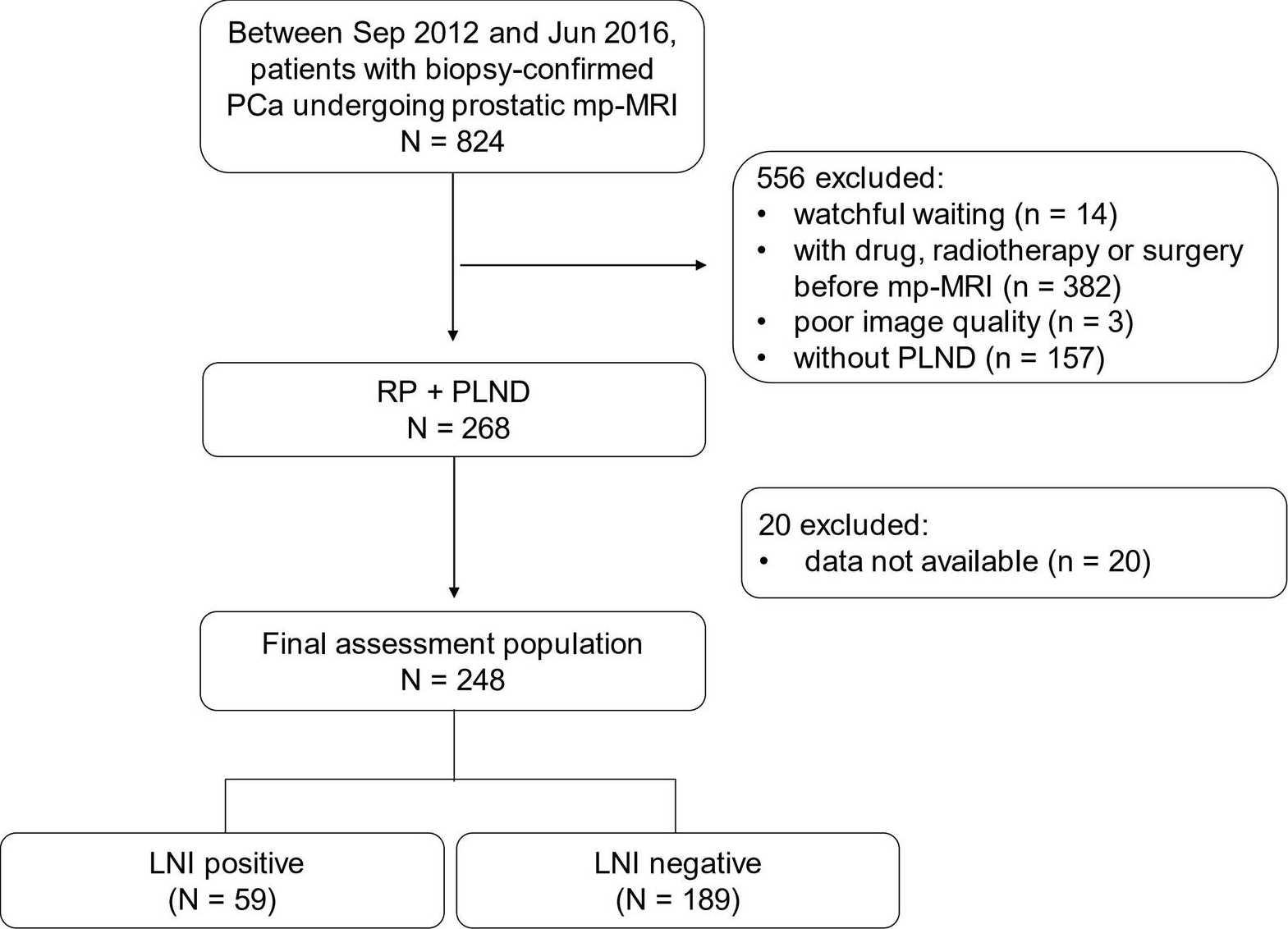
Fig. 1: Flowchart of the study population.
Note: mp-MRI= multi-parametric magnetic resonance imaging. PLND = pelvic lymph node dissection. LNI = lymph
node invasion. PCa= prostate cancer.
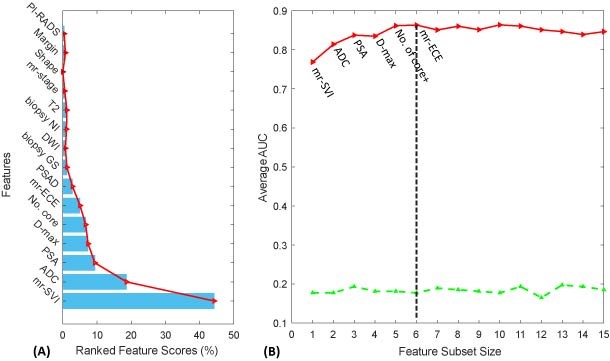
Fig. 2: Results of
feature selection, feature ranking and model construction with Recursive Feature Elimination-
Support Vector Machine (RFE-SVM) analysis. (A) Distribution of weight
for Features with RFE analysis. (B) SVM classifier is trained by adding ranked
feature one-by-one. The iteration repeated until the desired number of features
was reached. The desired features and classifier parameters are selected to be
those resulting in best accuracy and least estimated bias over cross-validation
(dot line).
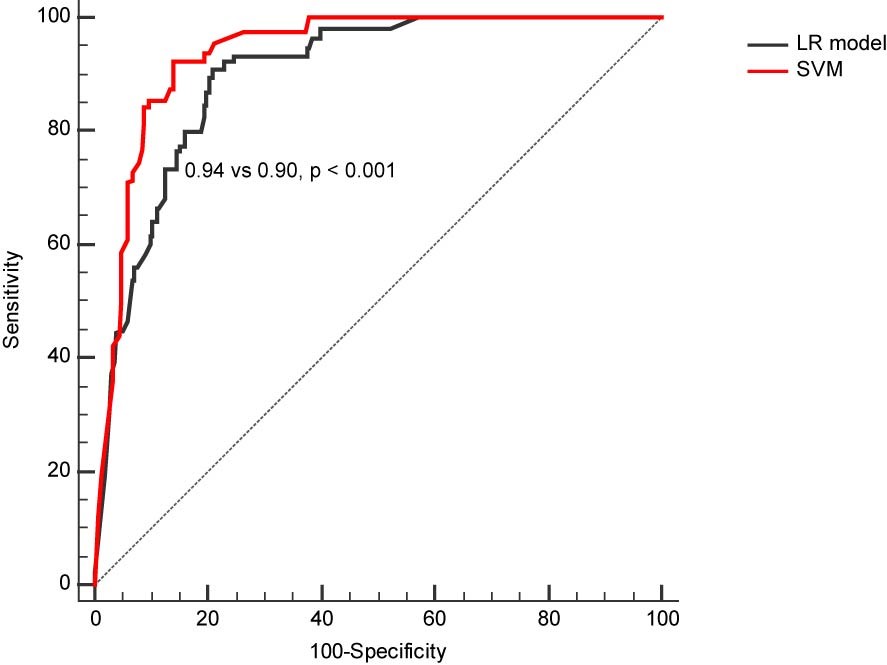
Fig. 3: Distribution of adjusted lymph
node
(LN) risk score between patients with and without Lymph
Node Invasion
(LNI) estimated by Logistic Regression (LR) model (A) and Support Vector
Machine (SVM) model (B).
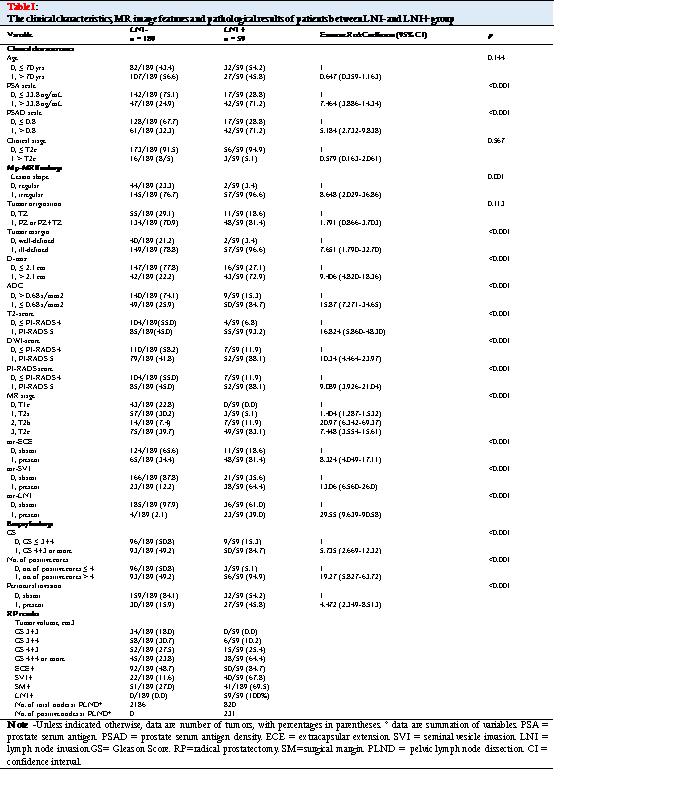
The clinical characteristics, MR image features and
pathological results of patients between LNI- and LNI+ group.
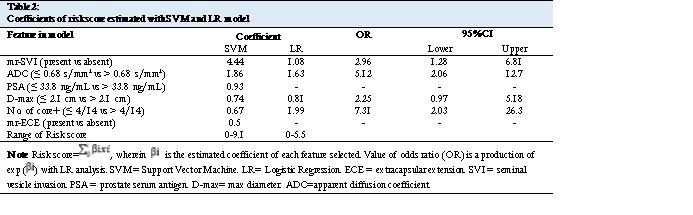
Coefficients of risk score estimated with SVM and LR model
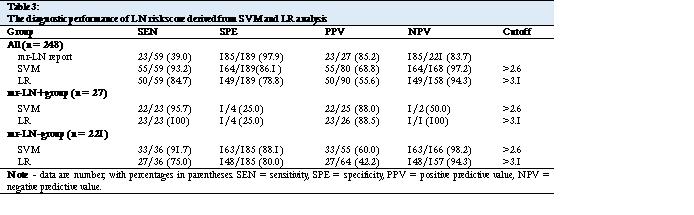
The diagnostic performance of LN risk score derived from SVM and LR analysis