1848
Probing Structure of Normal and Malignant Prostate Tissue before and after Radiation Therapy with Luminal Water Fraction and Diffusion-Weighted MRI1Cancer Research UK Imaging Centre, The Institute of Cancer Research, Sutton, United Kingdom, 2MRI Unit, The Royal Marsden Hospital NHS Foundation Trust, Sutton, United Kingdom
Synopsis
Luminal Water Fraction (LWF) is higher in peripheral than transitional zone of the untreated prostate; in comparison, it is significantly reduced in tumors. LWF is correlated with ADC in untreated non-malignant prostate. LWF is not correlated with ADC in tumors or in post irradiated prostate indicating that the morphological factors affecting LWF and ADC in these tissues are independent.
Background
Interpretation of diffusion-weighted (DW) in conjunction with T2-weighted MRI is essential for assessing prostate cancer. Although the Apparent Diffusion Coefficient (ADC) derived from DW imaging provides quantitative data, quantitative T2 mapping remains relatively unexplored. Prostate cancer grade progression results in increasing disruption of glandular structure and a gradual obliteration of the luminal space, so that the proportions of the short and long T2 components are likely to vary with histologic tumor grade; in fact the long T2 component, represented by the luminal water fraction (LWF), has been shown to correlate positively with the amount of luminal space1 and negatively with increasing Gleason grade2. Moreover, where glandular structure is destroyed post radiation, the role of T2 quantitation may have a role in distinguishing irradiated non-malignant tissue from disease recurrence.Aim
To quantify the T2 components, the ADC and the relationship between these parameters in untreated and irradiated non-malignant prostate tissue as a measure of glandular and cellular compartments and to compare the values with those from tumor.Methods
Twenty-four patients with biopsy-proven prostate cancer were imaged with an endorectal technique at 3T (Philips Achieva). 14 were untreated (ages 54-77 years, PSA 5.6 to 20.0 ng/mL, Gleason scores 3+3 in 9, 3+4 in 4 and 4+3 in 1 case) and 10 (aged 69-78 years, PSA 1.5-14 ng/ml), were treated with radiation therapy between 1-14 years previously. No evidence of tumor on MRI in 2 cases in the post-treatment group was confirmed by template biopsy. DW-MRI (b-values of 0, 25, 50, 75, 100, 300, 500 and 800 s mm−2) and T2 multi-echo GRASE (32 echoes, range 25-800 ms) were acquired axially. Regions of interest (ROI) were drawn on T2-weighted images and ADC maps derived from monoexponential fits of b100-800. Mono- and bi-exponential models were fitted to the multi-echo T2 images assuming Rician image noise, and the Bayesian information criterion was used to select the model in each voxel in order to generate LWF, T2 short and T2 long maps3. Parameter values for LWF, T2 short and T2 long were compared between tissue types using the Wilcoxon rank-sum test.Results
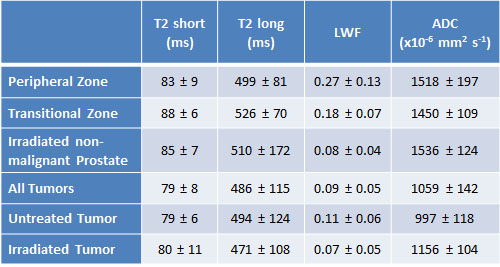
The LWF was significantly higher in the peripheral zone (PZ) than in the transitional one (TZ) in line with the predominant glandular structure of the formenr. In addition, the LWF of irradiated prostate showed values significantly lower than untreated PZ (p=10-5) or TZ (p=10-6) (Table 1). However, comparison of the short and long T2 elements between untreated and irradiated prostate indicated no differences. ADC values of untreated PZ, TZ and irradiated non-malignant prostate also did not show significant differences.
In normal untreated (pooled PZ and TZ) prostate tissue, there was a strong correlation between LWF and ADC (r=0.82, p<0.001) and a weak correlation between T2 short and ADC (r=0.49, p<0.01). No relationship was observed between LWF and ADC in irradiated prostate.
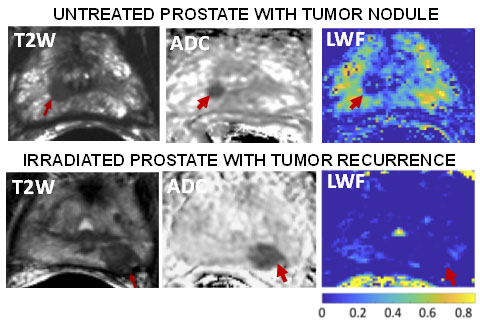
In tumor tissue, LWF was significantly lower than in normal PZ and TZ tissue (p<0.01 in both cases), but not than irradiated prostate tissue (Figure 1). LWF and ADC were not correlated in tumors (r=-0.05, p=0.88).
Discussion and Conclusions
The loss of LWF in the irradiated prostate is consistent with the known effect of radiation on glandular function. Moreover, the relationship between LWF and ADC that is evident in untreated non-malignant prostate tissue is disrupted after radiation therapy. This reflects the fact that the measured MR parameters are influenced by independent morphological features in irradiated tissue. LWF was strikingly different between non-malignant and tumor tissue in the untreated prostate, where it potentially would be a useful adjunct to ADC in prostate cancer assessment. As there was no significant difference in LWF between irradated non-malignant tissue and tumor, LWF is unlikely to be useful in delineating recurrent tumor in the irradiated gland.Acknowledgements
CRUK support to the Cancer Imaging Centre at ICR and RMH in association with MRC and Department of Health C1060/A10334, C1060/A16464 and NHS funding to the NIHR Biomedical Research Centre and the Clinical Research Facility in Imaging.References
1. Sabouri S, Fazli L, Chang SD, Savdie R, et al. MR measurement of luminal water in prostate gland: Quantitative correlation between MRI and histology. Journal of magnetic resonance imaging : JMRI. 2017;46(3):861-9.
2. Sabouri S, Chang SD, Savdie R, et al. Luminal Water Imaging: A New MR Imaging T2 Mapping Technique for Prostate Cancer Diagnosis. Radiology. 2017;284(2):451-9.
3. Carlin D, Orton M, Morgan VA, et al. A comparison of biexponetial fitting and spectral modelling methods for T2 mapping of prostate cancer. Proc. Intl. Soc. Mag. Reson. Med. 26 (2018)
Figures