1845
The apical surgical margin status prediction of prostate cancer based on radiomics analysis derived from T2-weighted imaging: Clinical implementation1Peking University First Hospital, Beijing, China
Synopsis
This retrospective study aims to validate a computer-aided diagnosis (CAD) system based on radiomics analysis in predicting the apical surgical margin (SM) status before radical prostatectomy (RP). 81 patients who received preoperative prostate T2-weighted MR imaging were evaluated by the CAD system and experienced radiologists, according to the sign of extracapsular extension (ESE), using pathological findings as a reference standard. The resulting algorithm was then validated from another external dataset of 38 patients in the same way. The results demonstrated this CAD system performed well and might help radiologist and surgeons make appropriate decisions concerning RP surgical approaches.
Introduction
Given the importance of apical positive surgical margins (PSM) at radical prostatectomy (RP), many attempts to predict PSM have been tried. Recently, preoperative prostate MR scans have also been recommended to serve as a road map for surgery, with increasing values going beyond simply detecting or staging the tumors1. Computer-aided diagnosis systems based on radiomics analysis showed potential to identify patients at high risk of PSM preoperatively and presented a need to be validated for clinical implentation2.Objective
To develop and validate a CAD system based on radiomics analysis derived from T2-weighted images for preoperatively predicting the apical surgical margin status.Methods
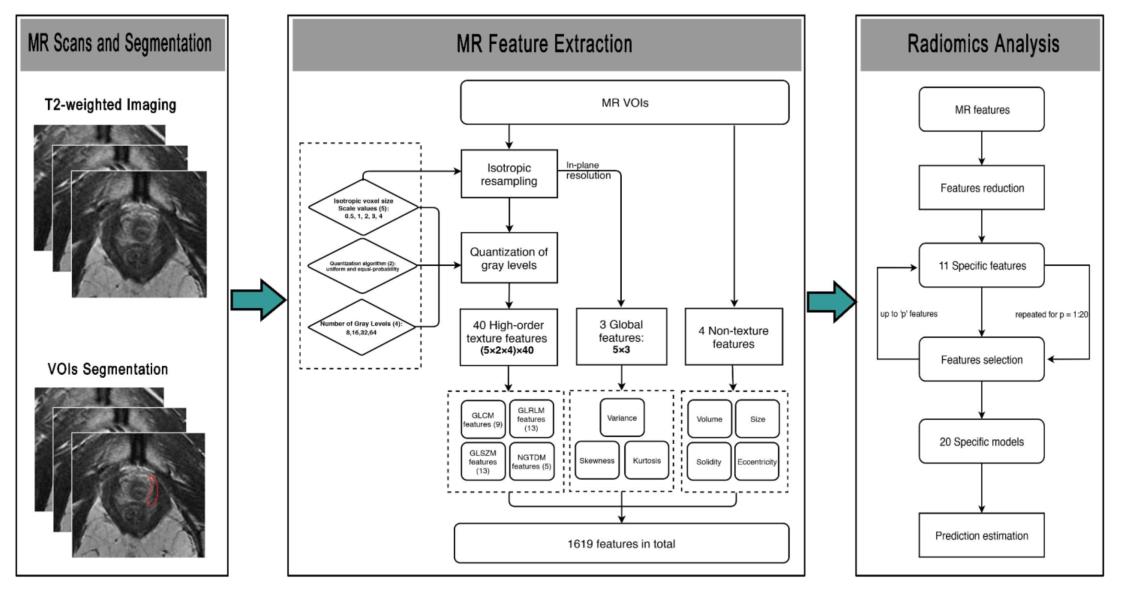
Institutional review board (IRB) approval was obtained for this retrospective study, with waiver of informed consent. Between September 2013 and June 2018, a total of 119 patients (training cohort: n = 81; testing cohort, n = 38) with 238 bilateral pathological confirmed bilateral apical margin status (162 margins in training set and 79 margins in testing set, a total of 76 positive and 162 negative cases) were reviewed. T2-weighted imaging were performed before the radical prostatectomy (RP). In all, four non-texture features and 1,615 radiomics features were extracted for each surgical margin (Fig. 1). Based on multivariate logistic regression with bootstrapping approach, the selected features were used to construct the predictive radiomics model (Fig. 2). In addition, two experienced radiologists respectively interpreted the validation dataset of 76 surgical margins in terms of the sign of extracapsular extension (ESE), which is associated with positive SM and has been confirmed as a promising predictor of SM positivity. Interobserver agreement on the MR-reported ESE were performed and the consensus results achieved were compared with the predictive outcome of the radiomics model. The predictive performance was evaluated by area under the receiver-operating characteristic curves (AUC). The pathological findings were used as the reference standard.Results
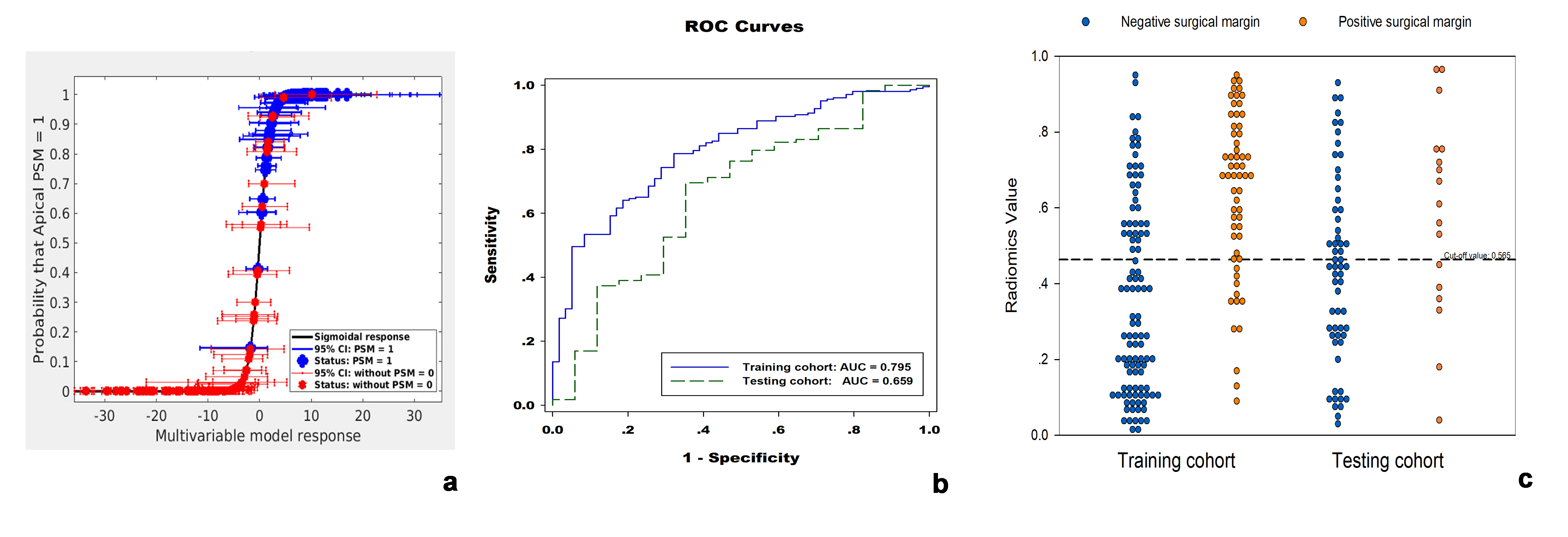
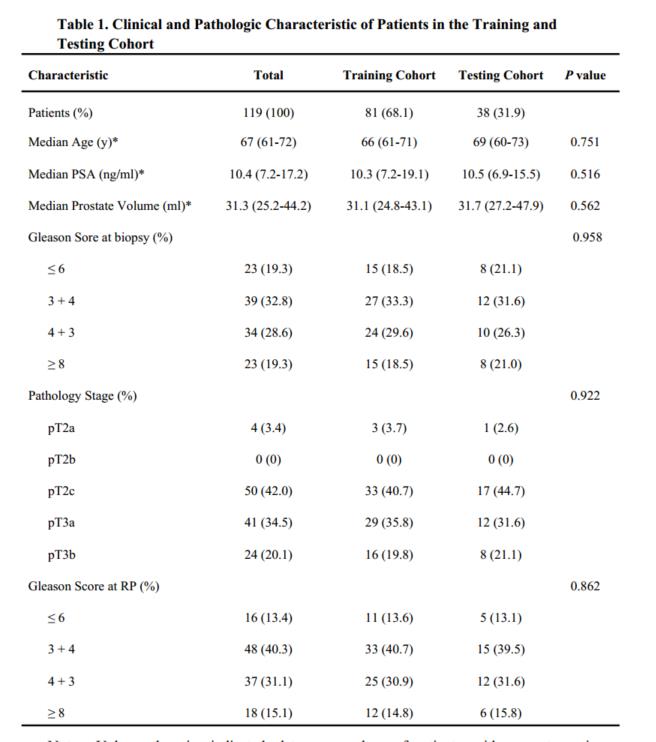
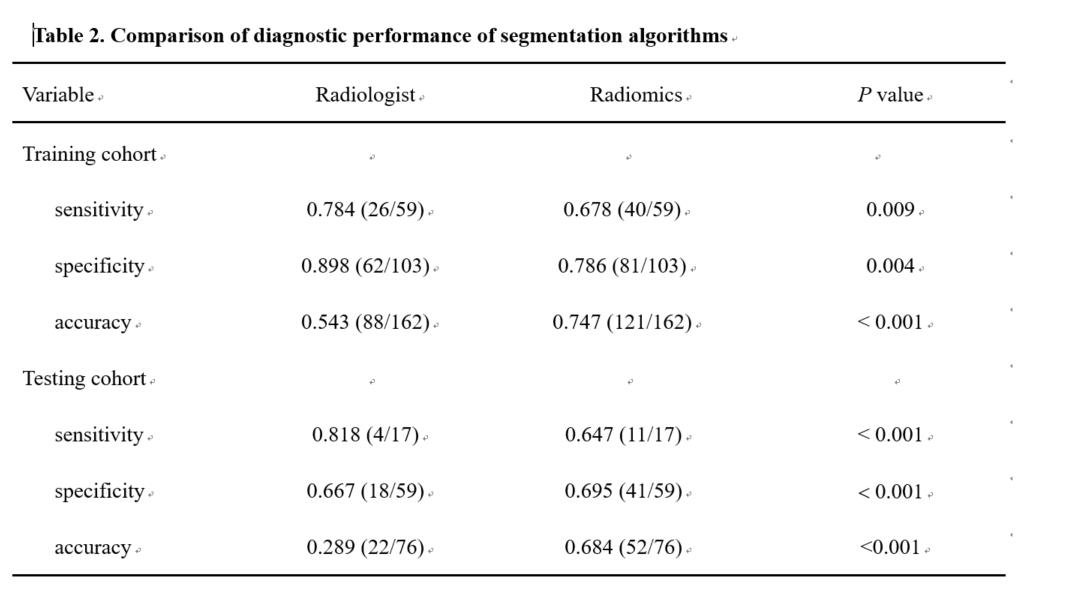
In the current study, the basic characteristic of patients were listed in Table 1. The radiomics model, with eleven selected optimal features, reached the AUC of 0.795 in the training set, with the sensitivity, specificity of 0.678, 0.786, and 0.747, respectively. Besides, in the testing cohort, the model yielded the AUC of 0.647, with the sensitivity, specificity, and accuracy of 0.647, 0.695, and 0.660, respectively. For the recognition of MR-reported ESE signs, interobserver agreement were substantial for the two experienced radiologists (k = 0.72 and k = 0.70 for the training cohort and testing cohort, respectively). However, compared with the radiologists’ performance (Table 2), the CAD system showed a higher performance concerning the AUC, sensitivity, specificity and accuracy, with statically significance difference (all P < 0.05).Discussion
In the current study, although substantial agreements were achieved from the radiologists, the diagnostic performance demonstrated lower in predicting the apical surgical margins status, showing the challenging in identification of ESE on the MR images. This result is understandable, that correct recognition of ESE could also be challenging even at pathology for the misinterpreting desmoplastic and fibrotic reaction as organ-confined disease. However, the implication of CAD based on radiomics analysis could get the more objective and reliable results than the macroscopic MR reported signs.Conclusion
It demonstrated that the validated CAD system based on radiomics model derivered from T2-weighted images shows the potential to predict apical margin status, serving as a noninvasive biomarker for preoperative planning of the approach to RP and eventually improving the personalized treatment.Acknowledgements
No acknowledgement found.References
1. McEvoy SH, Raeside MC, Chaim J, et al. Preoperative Prostate MRI: A Road Map for Surgery. AJR American journal of roentgenology 2018;211(2):383-391.
2. Stoyanova R, Takhar M, Tschudi Y, et al. Prostate cancer radiomics and the promise of radiogenomics. Translational cancer research 2016;5(4):432-447.
Figures