1844
Accuracy of IMPROD biparametric pre-biopsy MRI for prostate cancer detection in correlation with whole mount prostatectomy sections: implications for focal therapy (IMPROD trial, #opensourcetrial)1University of Turku, Turku, Finland, 2Turku University Hospital, Turku, Finland, 3Icahn School of Medicine at Mount Sinai, New York, NY, United States
Synopsis
In this prospective single institutional trial(NCT01864135), we evaluated the accuracy of a unique prostate MRI acquisition and reporting protocol, IMPROD biparametric MRI, in men with a clinical suspicion of prostate cancer who were subsequently diagnosed with prostate cancer and underwent prostatectomy. IMPROD biparametric MRI correctly detected 75% (75/99) of prostate cancer lesions with diameter ≥5 mm or any Gleason grade 4, and only two of the missed prostate cancer lesions had Gleason score >3+4. However, only a limited accuracy on isotropic voxel level was achieved potentially limiting focal therapy planning. All data are freely are available at the following address: http://petiv.utu.fi/improd
INTRODUCTION
The IMPROD clinical trial (1,2) (NCT01864135, IMPROved prostate cancer Diagnosis – combination of Magnetic Resonance Imaging and biomarkers; http://mrc.utu.fi/mri/improd) was designed to evaluate performance of a novel unique rapid MRI protocol, IMPROD biparametric MRI (bpMRI) protocol, and selected biomarkers in men with a clinical suspicion of PCa based on elevated PSA. In this sub-analysis we explored the accuracy of IMPROD bpMRI for PCa detection on voxel level with special attention to focal therapy planning using IMPROD bpMRI which is a faster and less expensive MRI protocol than commonly used MRI protocols (1,3–5).METHODS
IMPROD bpMRI was performed using a 3T MR scanner and surface array coils. T2-weighted (T2w) imaging in axial and sagittal planes was performed followed by diffusion weighted imaging (DWI) collected in three separate acquisitions: 1. repetition time/echo time (TR/TE) 5543/80 ms, b-values 0, 100, 200, 300, 500 s/mm2, acquisition voxel size 2.0×2.0×3.0mm3, no intersection gaps (4); 2. TR/TE 5000/87 ms b-values 0, 1500 s/mm2, acquisition voxel size 2.0×2.0×5.0mm3, no intersection gaps, 3. TR/TE 5000/87 ms, b values 0, 2000 s/mm2, acquisition voxel size 2.0×2.0×5.0mm3, no intersection gaps. An importable version of the MRI acquisition protocol is freely publicly available at the trial server (http://petiv.utu.fi/improd).
Before initialization of the trial (2010-2013), a dedicated system for reporting (IMPROD Likert scoring system) was developed (4,6). IMPROD bpMRI examinations, including manual lesion delineations, were prospectively reported by one reader. Suspicious lesions on IMPROD bpMRI were delineated manually on axial T2w images using integrated information from all bpMRI data sets without knowledge of clinical or laboratory parameters such as prostate specific antigen level. The lesion extent was determined by the largest signal abnormality seen on T2w imaging or the separate three DWI acquisitions. Following completion of the trial, Prostate Imaging Reporting and Data System version 2 (PI-RADSv2) scores were assigned (7). In men who underwent prostatectomy, the hematoxylin-eosin stained whole mount sections were prepared as previously described (8,9). Whole mount prostatectomy sections were matched with in-vivo T2w images based on anatomical landmarks such as location of benign prostatic nodules and shape of urethra. Only PCa lesions with diameters ≥5 mm or any Gleason grade 4 were included in final analyses. All hematoxylin-eosin stained histological slides are freely available at the following address: http://petiv.utu.fi/improd
Sensitivity, specificity, and accuracy of prospectively reported manual cancer delineations were evaluated on voxel level using three different voxel sizes: 1. reconstruction voxel size of axial T2w images 0.625 x 0.625 x 3.0 mm3 (voxel volume of 1.17 mm3); 2. interpolated isotropic voxel size of 1.0 x 1.0 x 1.0 mm3 (volume of 1 mm3); 3. interpolated isotropic voxel size of 5.0 x 5.0 x 5.0 mm3 (volume of 125 mm3). Finally, sensitivity, specificity, and accuracy were estimated on 36 region-of-interest level(10). In addition to evaluation of the prospectively reported manual cancer delineations, these manual delineations were increased by 5 mm and 10 mm using the nearest neighbour interpolation for binarized segmentation images in each direction to explore the effect of increasing size of manual cancer delineations on PCa detection sensitivity on voxel level. Finally, a region growing algorithm in all three directions(11) was used. Region growing algorithm was applied in three-dimensional (3D) iterative fashion with 3x3x3 dilation kernel to achieve sensitivity of 95% and 100% on voxel level for all IMPROD bpMRI detected PCa lesions (Figure 1).
RESULTS
One-hundred-seventy-five men were prospectively enrolled, 171/175 (97%) underwent bpMRI, 164/175 (94%) underwent biopsy and finally 64/175 (37%) underwent prostatectomy. The median time period between IMPROD bpMRI examination and prostatectomy was 110 days (interquartile range, 95 - 136 days). Table 1 summarizes the patient demographics.
In total, 99 PCa lesions were identified (Table 2), 40 (40%, 40/99) with Gleason score (GS) >3+4. Twenty-four PCa lesions (24%, 24/99) were missed by IMPROD bpMRI, two (5%, 2/40) with GS >3+4 (Figure 2). All dominant PCa lesions were correctly diagnosed using IMPROD bpMRI. 3D dilation of manual cancer delineations in all directions by approximately 10-12 mm was needed to achieve close to 100% sensitivity on voxel level (Table 3, Table 4, Figure 1).
The main limitation is uncertainty in co-registration accuracy of whole mount prostatectomy sections to in-vivo MRI.
DISCUSSION / CONCLUSION
Prebiopsy IMPROD bpMRI enabled the detection of 95% (38/40) of lesions with Gleason score >3+4. However, only limited accuracy on isotropic voxel was achieved potentially limiting focal therapy planning. Increasing PCa manual delineations by approximately 10-12 mm in all directions led to sensitivity approaching 100% for majority of IMPROD bpMRI detected lesions.Acknowledgements
This study was financially supported by grants from the Instrumentarium Research Foundation, Sigrid Jusélius Foundation, Turku University Hospital, TYKS-SAPA research fund, Finnish Cancer Society, Finnish Cultural Foundation, and Orion Research Foundation.References
1. Jambor I, Boström PJ, Taimen P, et al. Novel biparametric MRI and targeted biopsy improves risk stratification in men with a clinical suspicion of prostate cancer (IMPROD Trial). J Magn Reson Imaging. 2017;46(4):1089–1095.
2. Alinezhad S, Väänänen RM, Tallgrén T, et al. Stratification of aggressive prostate cancer from indolent disease-Prospective controlled trial utilizing expression of 11 genes in apparently benign tissue. Urol Oncol Semin Orig Investig. Elsevier; 2016;34(6):255.e15-255.e22.
3. Weinreb J, Barentsz J, Choyke P, et al. PI-RADS Prostate Imaging-Reporting and Data System:2015, Version 2. Eur Urol. 2016;69(1)(Version 2):16–40.
4. Jambor I, Kähkönen E, Taimen P, et al. Prebiopsy multiparametric 3T prostate MRI in patients with elevated PSA, normal digital rectal examination, and no previous biopsy. J Magn Reson Imaging. 2015;41(5):1394–1404.
5. Jambor I. Optimization of prostate MRI acquisition and post-processing protocol: a pictorial review with access to acquisition protocols. Acta Radiol Open. 2017;6(12):205846011774557.
6. Jambor I, Merisaari H, Taimen P, et al. Evaluation of different mathematical models for diffusion-weighted imaging of normal prostate and prostate cancer using high b-values: A repeatability study. Magn Reson Med. 2015;73(5):1988–1998.
7. Barentsz JO, Weinreb JC, Verma S, et al. Synopsis of the PI-RADS v2 Guidelines for Multiparametric Prostate Magnetic Resonance Imaging and Recommendations for Use. Eur Urol. European Association of Urology; 2016;69(1):41–49.
8. Jambor I, Borra R, Kemppainen J, et al. Functional Imaging of Localized Prostate Cancer Aggressiveness Using 11C-Acetate PET/CT and 1H-MR Spectroscopy. J Nucl Med. 2010;51(11):1676–1683.
9. Jambor I, Borra R, Kemppainen J, et al. Improved detection of localized prostate cancer using co-registered MRI and 11C-acetate PET/CT. Eur J Radiol. 2012;81(11):2966–2972.
10. Barentsz J, Villers A, Schouten M. Reply to Letter to the Editor re: ESUR prostate MR guidelines. Eur Radiol. 2013;23(8):2322–2323.
11. Oliphant TE. Python for Scientific Computing. Comput Sci Eng. 2007;9(3):10–20.
Figures
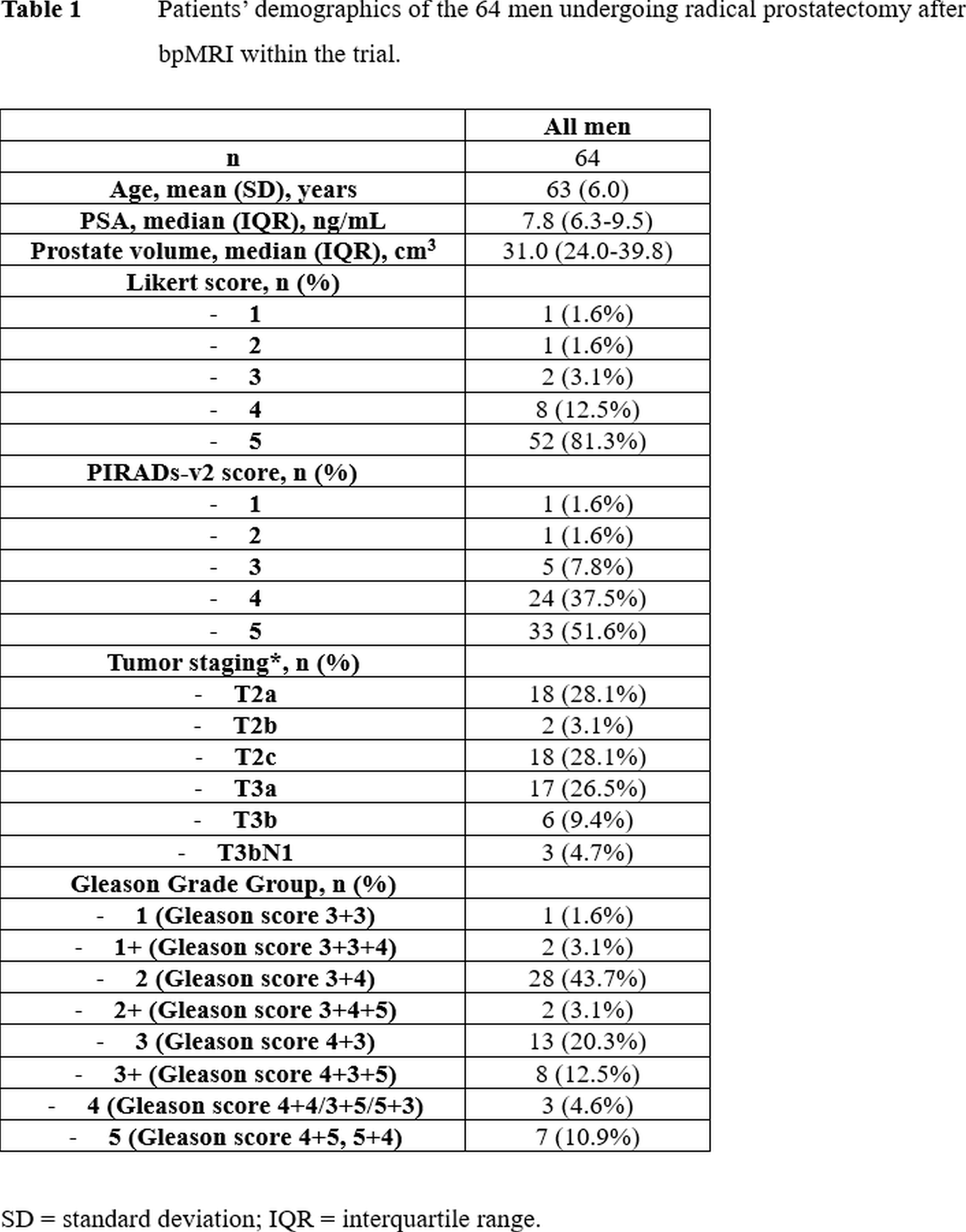
Table 1
Patients’ demographics of the 64 men undergoing radical prostatectomy after bpMRI within the trial.
SD = standard deviation
IQR = interquartile range
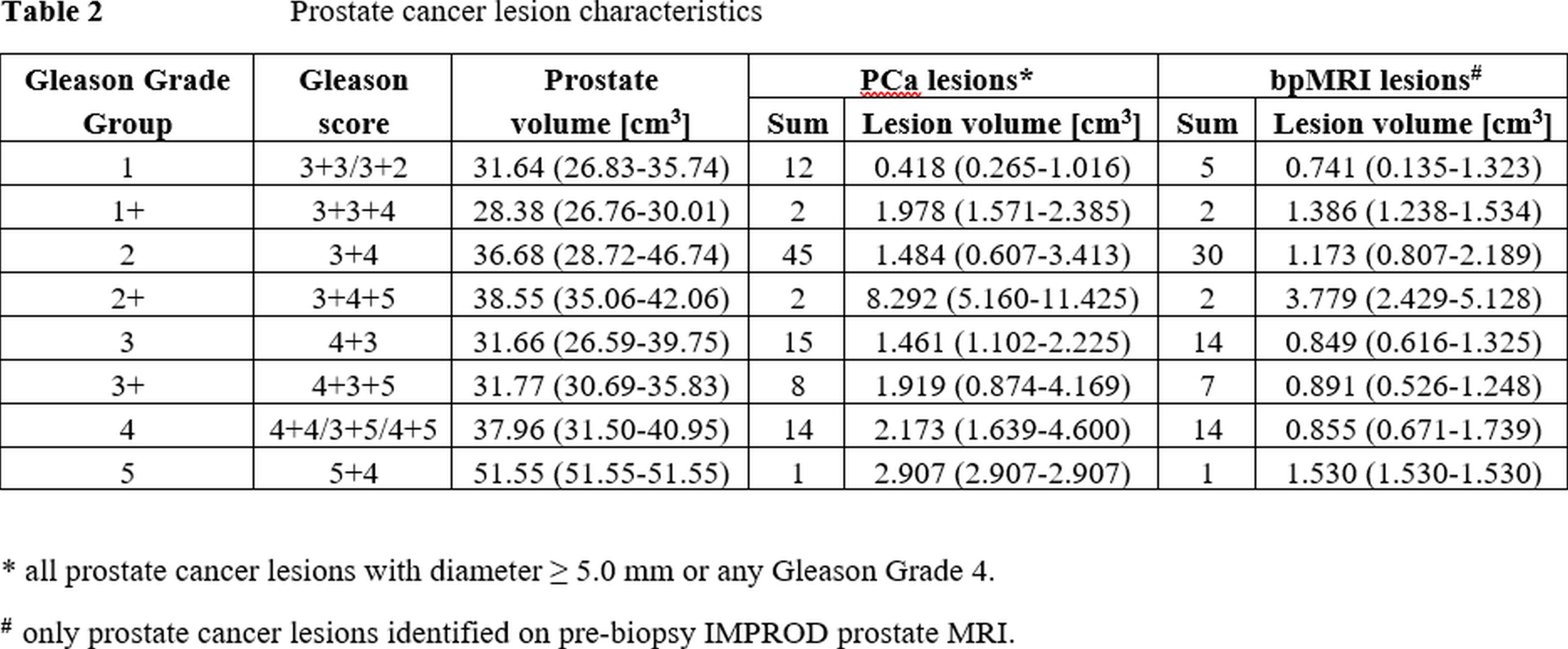
Table 2
Prostate cancer lesion characteristics.
* all prostate cancer lesions with diameter ≥ 5.0 mm or any Gleason Grade 4. # only prostate cancer lesions identified on pre-biopsy IMPROD prostate MRI.
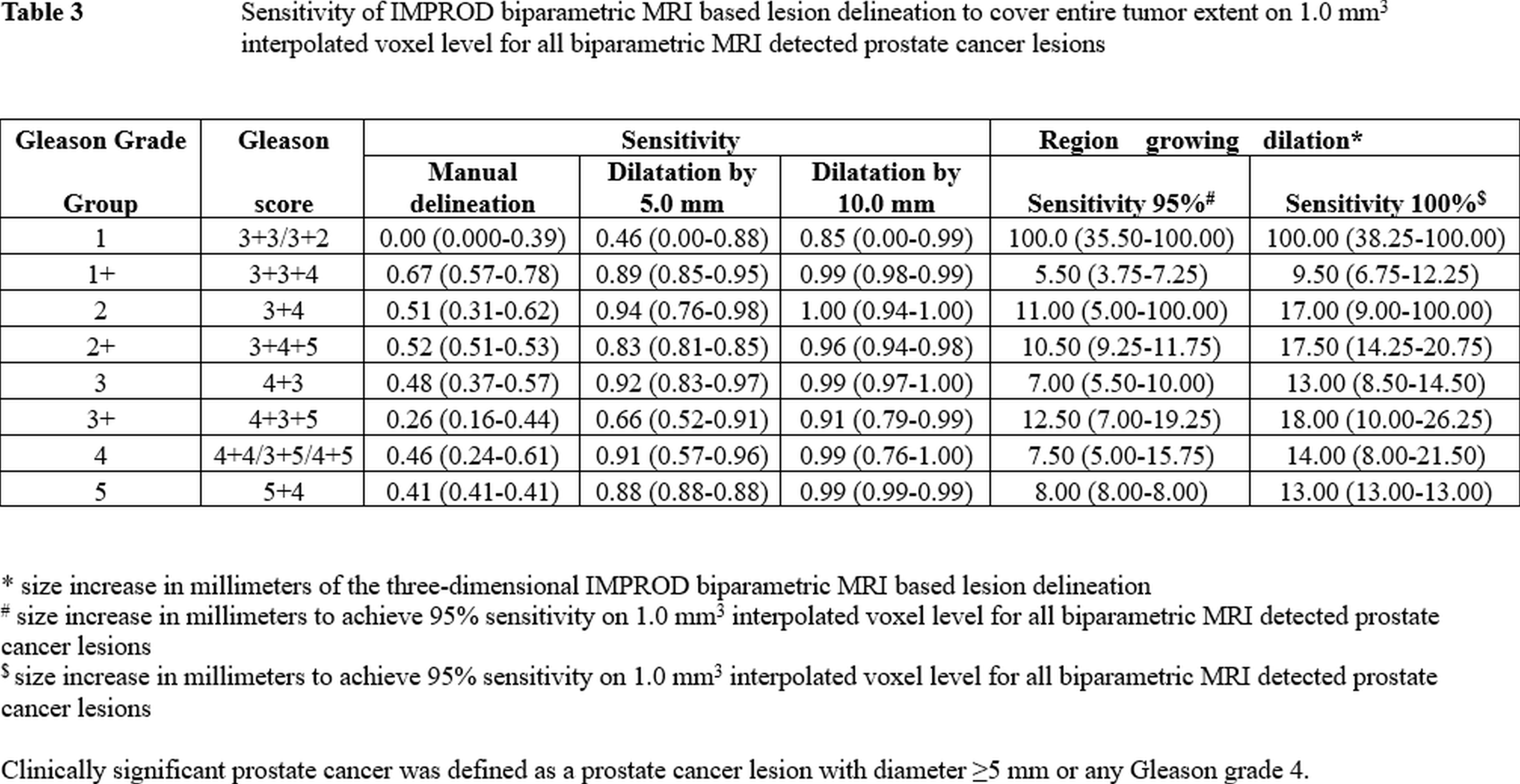
Table 3
Sensitivity of IMPROD biparametric MRI based lesion delineation to cover entire tumor extent on 1.0 mm3 interpolated voxel level for all biparametric MRI detected prostate cancer lesions.
* size increase in millimeters of the three-dimensional IMPROD biparametric MRI based lesion delineation # size increase in millimeters to achieve 95% sensitivity on 1.0 mm3 interpolated voxel level for all bpMRI detected prostate cancer lesions
$ size increase in millimeters to achieve 95% sensitivity on 1.0 mm3 interpolated voxel level for all bpMRI detected prostate cancer lesions
Only PCa lesions with diameter ≥5 mm or any Gleason grade 4 were included.
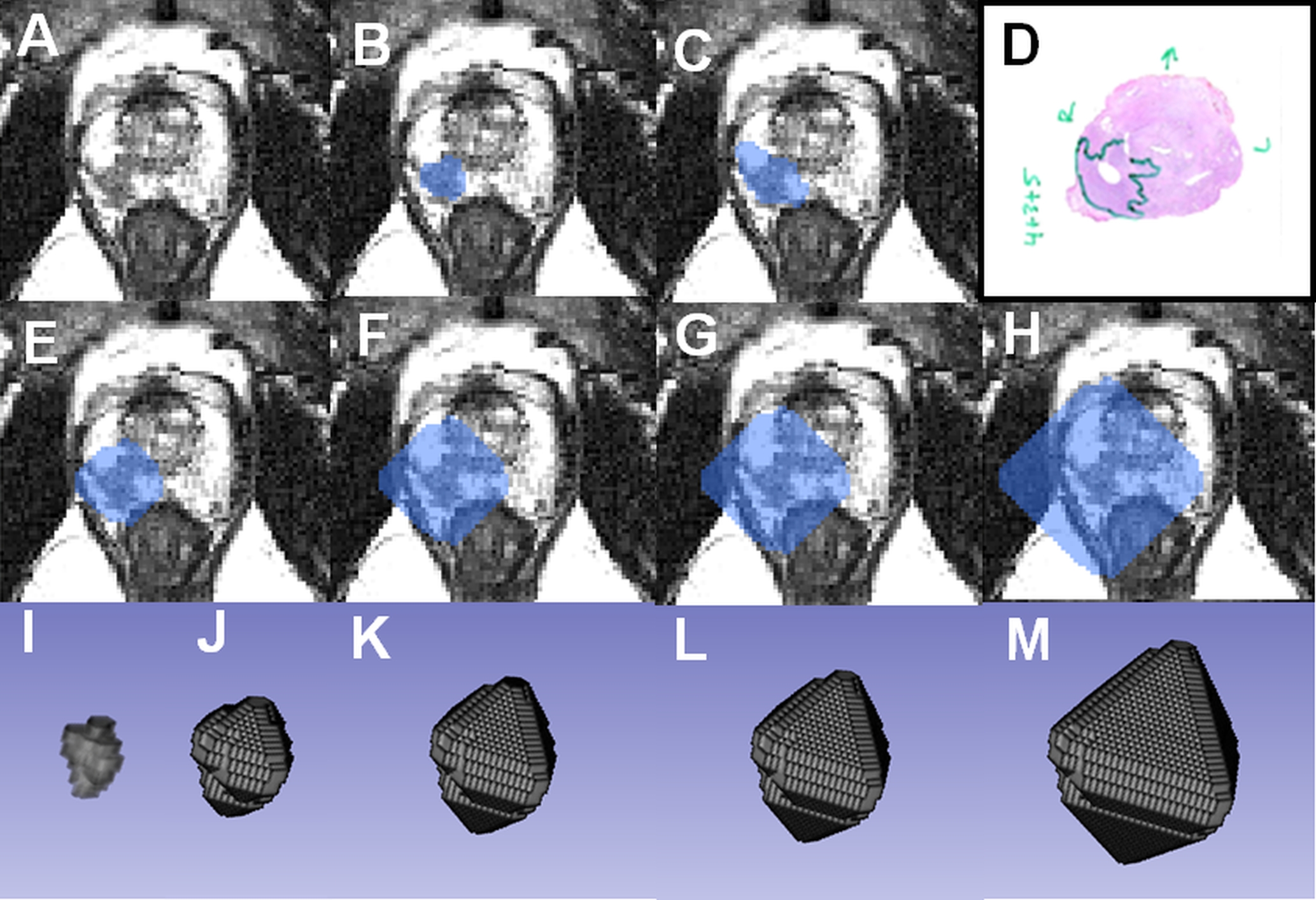
Figure 1
IMPROD patient number 45 (http://petiv.utu.fi/improd): Axial T2-weighted image with 1.0 x 1.0 x 1.0 mm3 voxel size (A), with overlaid IMPROD bpMRI based delineation (B) and whole mount prostatectomy based delineation (C). Prostate cancer is outline in green (D). Effect of increasing the lesion size by 5 mm (E) and 10 mm (F) is shown with the corresponding 3D volumes in J and K, respectively. The 3D volume of IMPROD bpMRI based delineation is shown in I as well as 3D volumes to achieve 95% sensitivity (G, L) and 100% sensitivity (H, M).
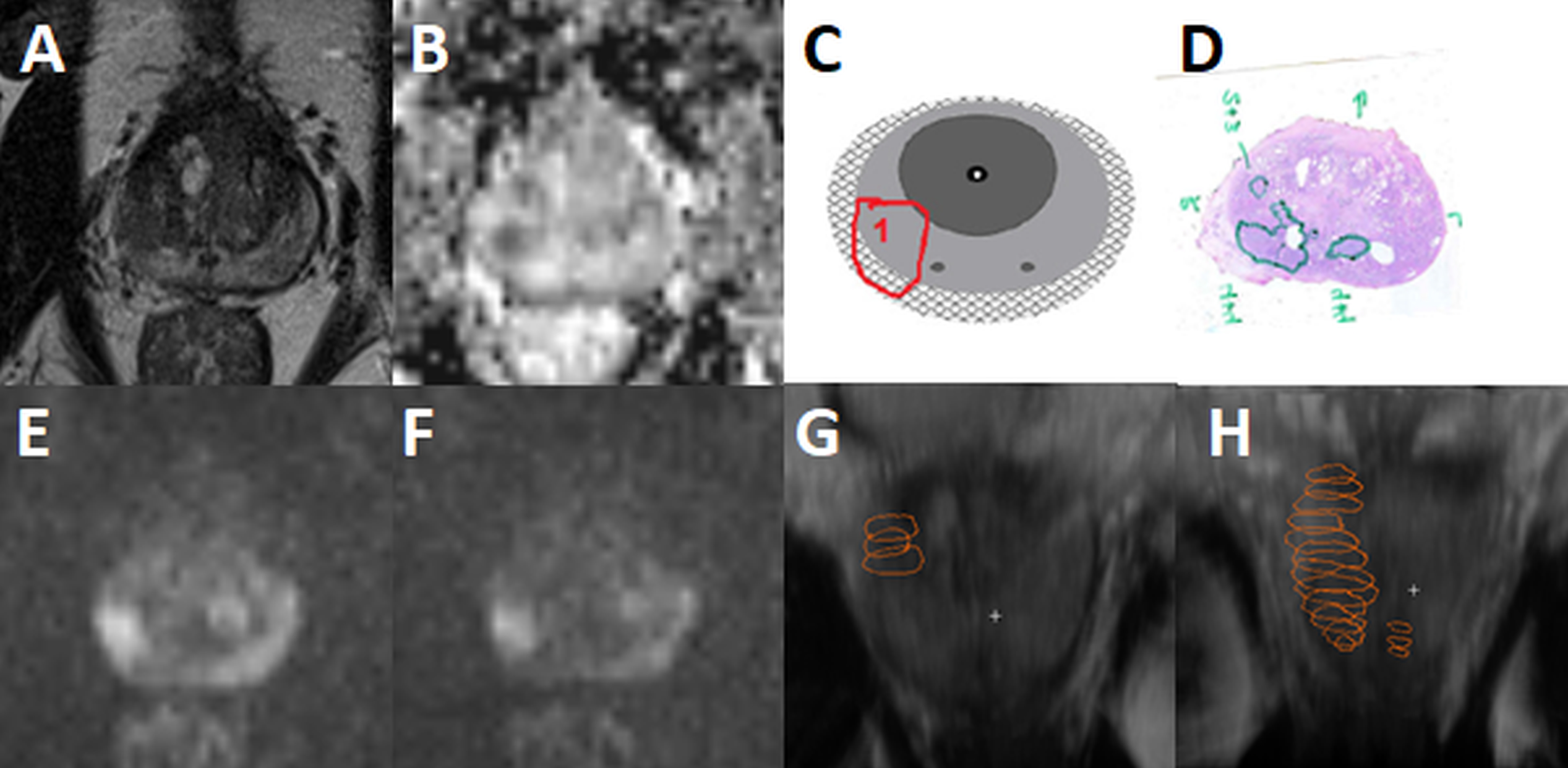
Figure 2
IMPROD patient number 21 (http://petiv.utu.fi/improd): IMPROD bpMRI Likert/Pirads 5/4 lesion in PZ with volume of 0.64 cm3. IMRPOD bpMRI detected lesion had Gleason score of 4+4 and size of 4.82 cm3. Smaller satellite Gleason score 4+4 (volume 0.18 cm3) lesion was missed by IMPROD bpMRI. Axial T2-weighted image (A), ADCm (5 b-values in the range of 0-500 s/mm2) (B), schematic drawing of the lesion (C), whole mount prostatectomy section (D), DWI b-1500 s/mm2 (E), DWI b-2000 s/mm2 (E), 3D-volume rendering of prospectively performed cancer delineation (G), and 3D-volume rendering of cancer delineation performed using whole mount prostatectomy sections(H).