1843
Prostate cancer detection in men with a clinical suspicion of prostate cancer using IMPROD biparametric MRI and expression of 11 genes (IMPROD trial, #opensourcetrial): evaluation using machine learning methods1University of Turku, Turku, Finland, 2Turku University Hospital, Turku, Finland, 3Icahn School of Medicine at Mount Sinai, New York, NY, United States
Synopsis
Eighty men with a clinical suspicion of prostate cancer (PCa) were enrolled as a part of IMRPOD trial (NCT01864135). The performance of 9 clinical parameters, 11 mRNA transcript levels and 4 IMPROD biparametric MRI (bpMRI) parameters for detection of PCa with Gleason score ≥3+4 was evaluated using GreedyRLS feature selection and nested cross-validation with area under the curve obtained from tournament leave-pair-out cross validation. IMPROD bpMRI reported using qualitative IMPROD Likert scoring system demonstrated high accuracy for PCa detection and none of the remaining parameters led to further improvement. All data are freely are available at the following address: http://petiv.utu.fi/improd
INTRODUCTION
Prostate multiparametric magnetic resonance imaging (MRI) is increasingly used as a triage test in men with an elevated prostate specific antigen (PSA). However, long acquisition time, high cost and inter-center/reader variability of a routine multiparametric prostate MRI continue to limit wider adoption. The IMPROD clinical trial(1,2) (NCT01864135, IMPROved prostate cancer Diagnosis – combination of Magnetic Resonance Imaging and biomarkers; http://mrc.utu.fi/mri/improd) was designed to evaluate performance of a novel unique rapid MRI protocol, IMPROD biparametric MRI (bpMRI) protocol, and the role of selected biomarkers in men with a clinical suspicion of PCa based on elevated PSA. The aim of this sub-study was to evaluate the diagnostic accuracy of IMPROD bpMRI and carefully selected molecular biomarkers in men with a clinical suspicion of prostate cancer (PCa) using advanced machine methods in an unbiased fashion. The selected 11 biomarkers were previously found to be up-regulated up to 1080-fold in histologically benign tissue from cancer harboring prostates compared with cystoprostatectomies samples without PCa(3–5).METHODS
In total, 164 men (Figure 1) with a clinical suspicion of PCa underwent IMPROD bpMRI (NCT02241122) using a 3T MR scanner and surface array coils. IMPROD bpMRI consists of T2-weighted imaging (T2w) and three separate epi read-out based diffusion weighted imaging (DWI) acquisitions (5 b-values 0-500 s/mm2, 2 b-values 0-1500 s/mm2, 2 b-values 0-2000 s/mm2). IMPROD bpMRI examinations were prospectively reported by one reader using an in-house developed IMPROD Likert scoring system. The probability of a suspicious lesion containing Gleason grade 4 was prospectively assigned based on the apparent diffusion coefficient (ADCm) maps calculated using a monoexponential fit and 5 b-values in the range of 0 to 500 s/mm2. This probability was expressed as DWI based Gleason grade score (DbGGS): 1. unlikely- ADCm above or equal to 850 x 10-6 mm2/s, 2. probable: ADCm below 850 x 10-6 mm2/s 3. highly probable- ADC below 750 x 10-6 mm2/s.
Men with Likert score 3-5 had two targeted biopsies (TBs) of the dominant lesion followed by 12-core systematic biopsy (SB) while men with Likert score 1-2 had only SB. Finally, two cores from normal-appearing prostate areas (based on IMPROD bpMRI) were obtained for the messenger RNA (mRNA) transcript levels of ACSM1, AMACR, CACNA1D, DLX1, PCA3, PLA2G7, RHOU, SPINK1, SPON2, TMPRSS2-ERG, and TDRD1 measured by quantitative reverse-transcription polymerase chain reaction (3–5). Following completion of the trial Prostate Imaging Reporting and Data System version 2 (PI-RADSv2) scores were assigned(6). Manual prostate delineations on T2w images were performed to calculate prostate volume. In addition, prostate volume was estimated using transrectal ultrasound (TRUS).
Following parameters were evaluated:
1. Clinical parameters (7): PSA, PSA density (dPSA) based on MRI and TRUS prostate volumes, free-to-total PSA (fPSA), digital rectal examination (DRE), use of 5α-reductase inhibitors (5-ARI), age, TRUS prostate volume, patient’s age.
2. mRNA transcript levels (11): ACSM1, AMACR, CACNA1D, DLX1, PCA3, PLA2G7, RHOU, SPINK1, SPON2, TMPRSS2-ERG, and TDRD1.
3. MRI parameters (4): IMPROD Likert, DbGGS, PI-RADSv2, MRI prostate volume.
Machine learning using GreedyRLS(7) feature selection and nested cross-validation was used to evaluate the performance of the parameters in detecting clinically PCa (SPCa), defined as Gleason score ≥3+4. The evaluation metric was the area under the curve (AUC) obtained from tournament leave-pair-out cross validation (TLPOCV)(8). Combination of SB and TB was used as “ground true” for model performance evaluation. IMPROD bpMRI acquisition protocol and all data is freely available at the following address: http://petiv.utu.fi/improd
RESULTS
In total, 80 (80/164, 49%) prospectively enrolled men were included in the final analyses (Figure 1). Patients’ demographics are summarized in Table 1. 76 men (95% 76/80) had no prior biopsy while 4 men (5% 4/80) had one prior negative systematic biopsy.
Feature selection using GreedyRLS and the clinical data showed that three features (fPSA, DRE and 5_ARI) have TLPOCV AUC of 0.83, an improvement compared with the best clinical feature (fPSA with AUC = 0.73) or using a linear regression model (RLS reg. paramenter=1) trained on all clinical features (TLPOCV AUC = 0.82). The same performance was achieved by linear regression using all clinical parameters and mRNA transcript levels (TLPOCV AUC = 0.82). Linear regression using all 24 features demonstrated TLPOCV AUC of 0.92. However, no features or combination of features outperformed IMPROD Likert score.
DISCUSSION / CONCLUSION
IMPROD bpMRI reported using qualitative IMPROD Likert scoring system demonstrated high accuracy for SPCa detection in men with a clinical suspicion of prostate cancer. None of the remaining 9 clinical parameters, 11 mRNA transcript levels and 3 IMPROD bpMRI derived parameters, led to further improvement.
All data is freely available at the following address: http://petiv.utu.fi/improd
Acknowledgements
This study was financially supported by grants from the Instrumentarium Research Foundation, Sigrid Jusélius Foundation, Turku University Hospital, TYKS-SAPA research fund, Finnish Cancer Society, Finnish Cultural Foundation, and Orion Research Foundation.References
1. Jambor I, Boström PJ, Taimen P, et al. Novel biparametric MRI and targeted biopsy improves risk stratification in men with a clinical suspicion of prostate cancer (IMPROD Trial). J Magn Reson Imaging. 2017;46(4):1089–1095.
2. Alinezhad S, Väänänen RM, Tallgrén T, et al. Stratification of aggressive prostate cancer from indolent disease-Prospective controlled trial utilizing expression of 11 genes in apparently benign tissue. Urol Oncol Semin Orig Investig. Elsevier; 2016;34(6):255.e15-255.e22.
3. Väänänen R-M, Lilja H, Kauko L, et al. Cancer-associated changes in the expression of TMPRSS2-ERG, PCA3, and SPINK1 in histologically benign tissue from cancerous vs noncancerous prostatectomy specimens. Urology. NIH Public Access; 2014;83(2):511.e1-7.
4. Alinezhad S, Väänänen R-M, Mattsson J, et al. Validation of Novel Biomarkers for Prostate Cancer Progression by the Combination of Bioinformatics, Clinical and Functional Studies. Kyprianou N, editor. PLoS One. Public Library of Science; 2016;11(5):e0155901.
5. Alinezhad S, Väänänen R-M, Ochoa NT, et al. Global expression of AMACR transcripts predicts risk for prostate cancer – a systematic comparison of AMACR protein and mRNA expression in cancerous and noncancerous prostate. BMC Urol. BioMed Central; 2016;16(1):10.
6. Barentsz JO, Weinreb JC, Verma S, et al. Synopsis of the PI-RADS v2 Guidelines for Multiparametric Prostate Magnetic Resonance Imaging and Recommendations for Use. Eur Urol. European Association of Urology; 2016;69(1):41–49.
7. Pahikkala T, Airola A, Salakoski T. Speeding up greedy forward selection for regularized least-squares. In Machine Learning and Applications (ICMLA), 2010 Ninth International Conference on (pp. 325-330). IEEE.
8. Montoya Perez I, Airola A, Boström PJ, et al. Tournament leave-pair-out cross-validation for receiver operating characteristic analysis. Stat Methods Med Res. 2018 Aug 20:962280218795190. doi: 10.1177/0962280218795190.
Figures
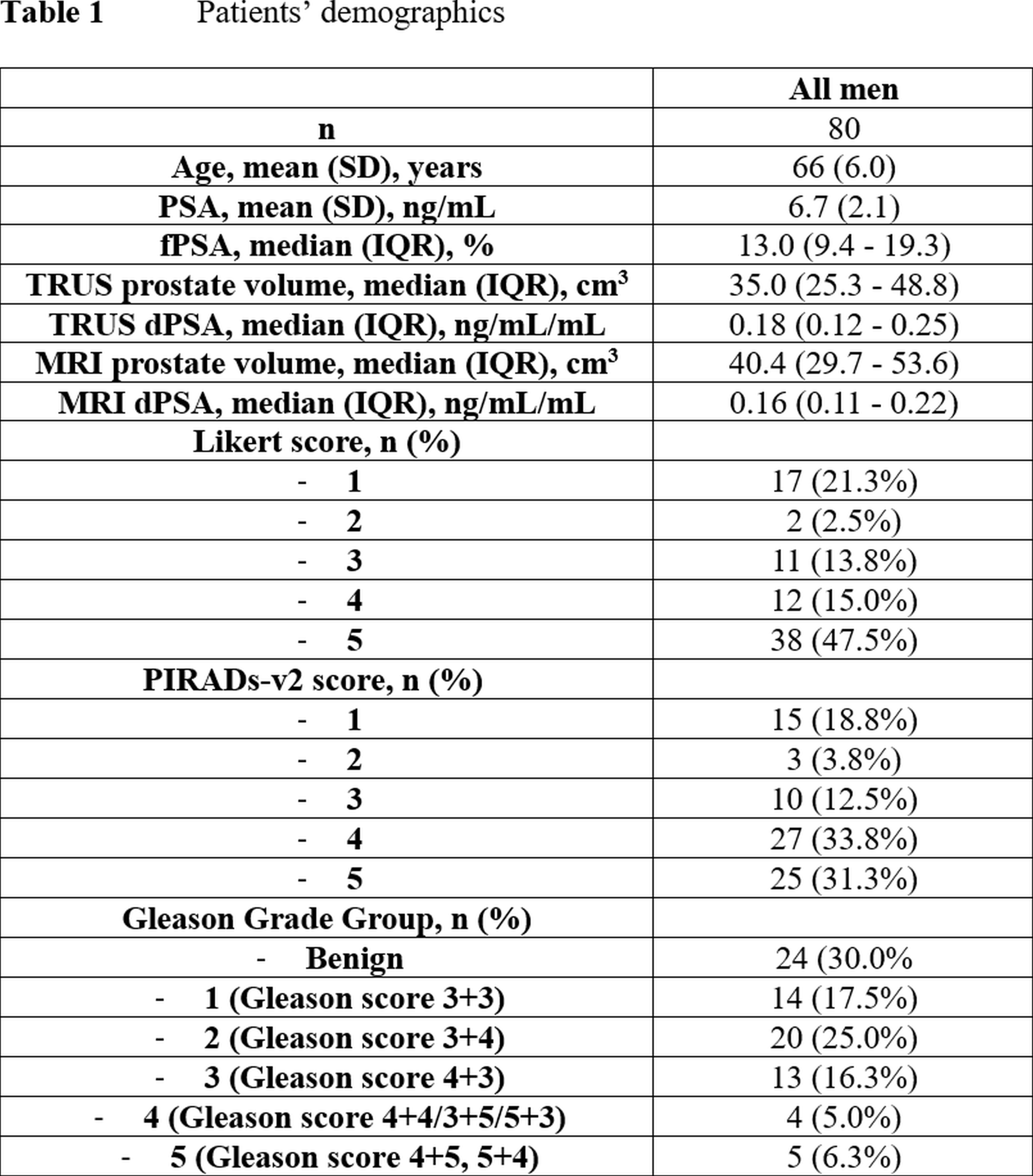
Table 1
Patients’ demographics
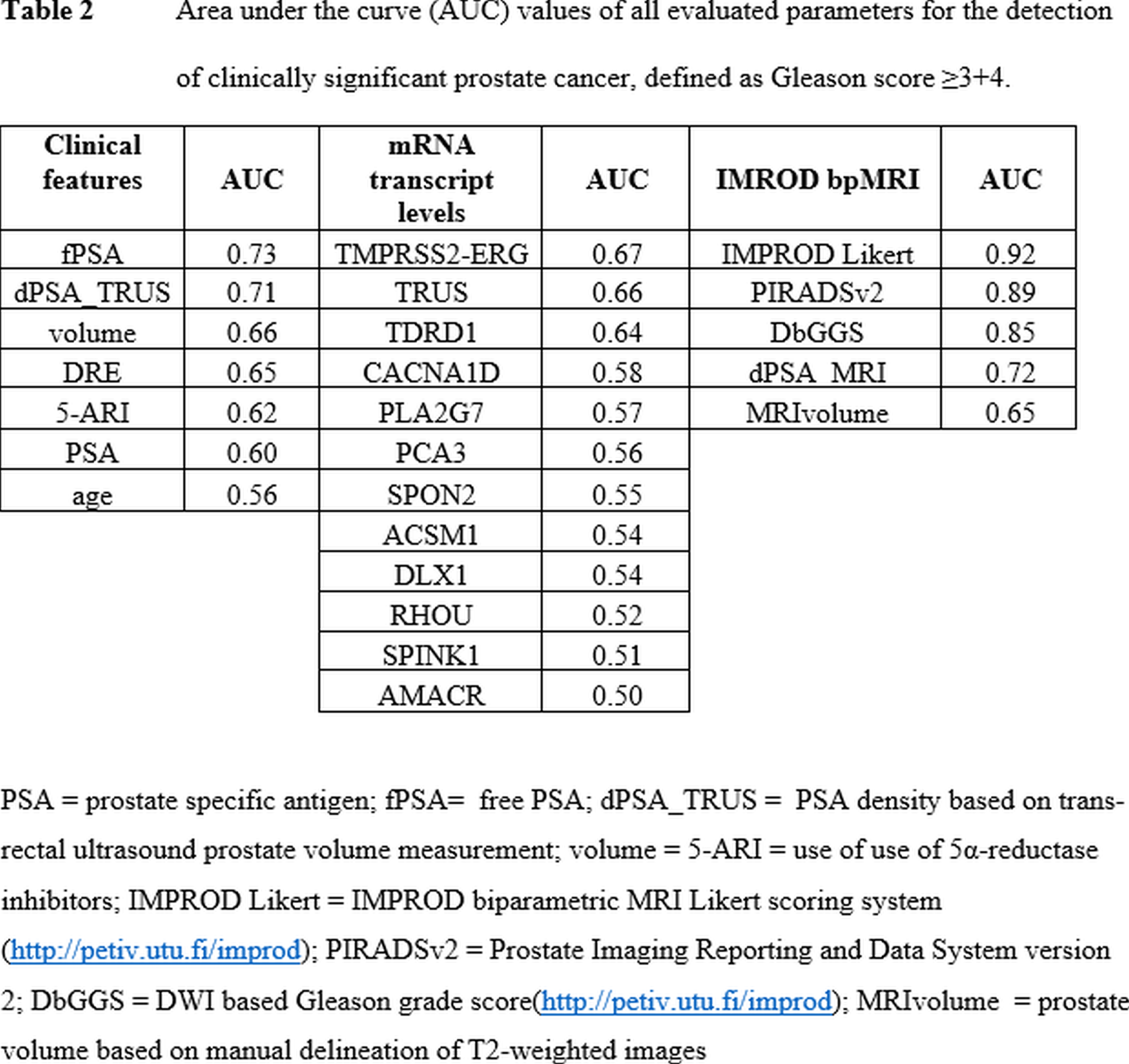
Table 2
Area under the curve (AUC) values of all evaluated parameters for the detection of clinically significant prostate cancer, defined as Gleason score ≥3+4.
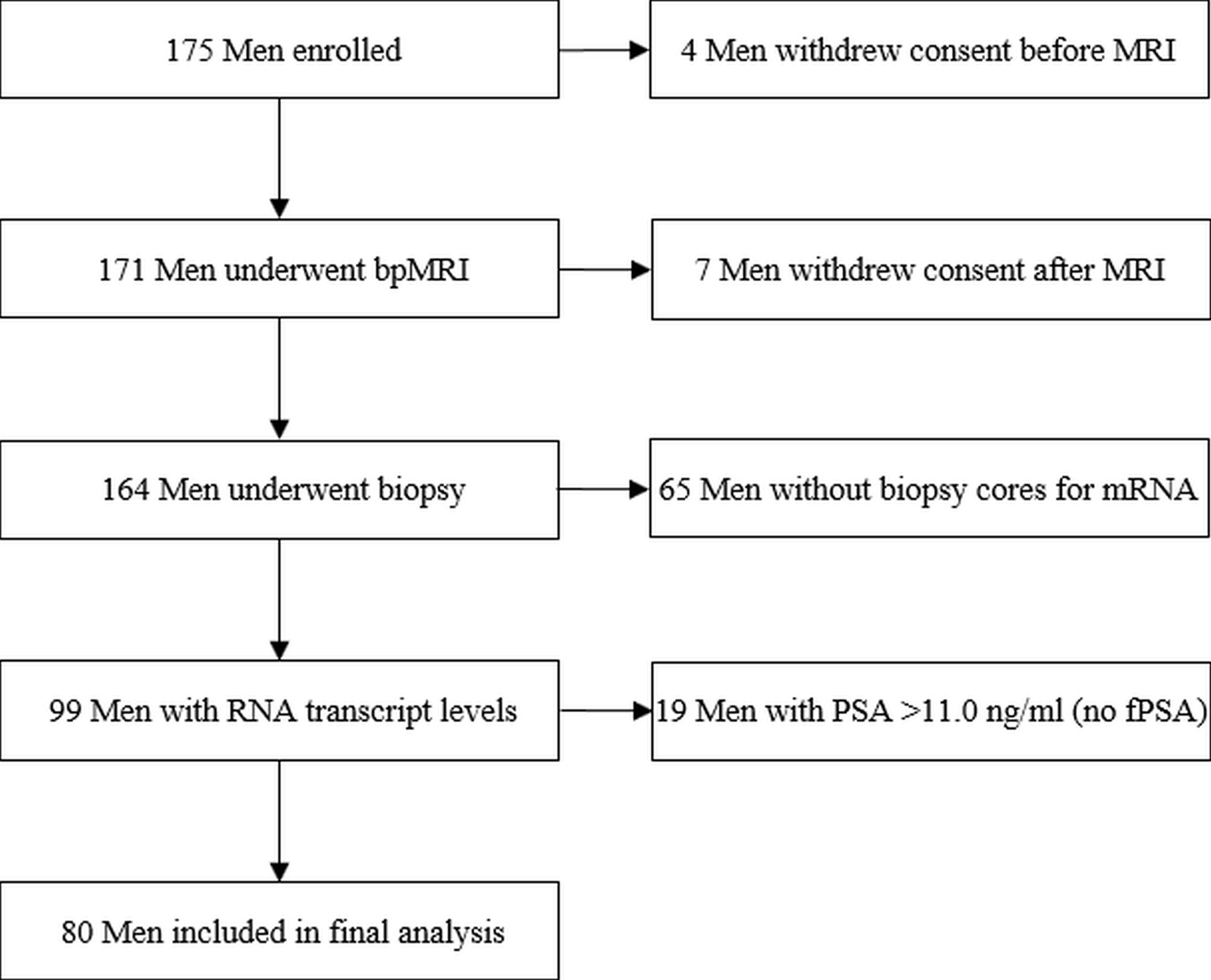
Figure 1
Study flow chart