1841
The Diagnostic Value of PI-RADS V2 Scoring System Combining with MRI-TRUS Fusion Targeted Biopsy for Detecting the Clinical Significant Prostate Cancer1The First Affiliated Hospital of Soochow University, SUZHOU, China, 2MR Scientific Marketing, Siemens Healthcare, Shanghai, SHANG HAI, China
Synopsis
Transrectal ultrasound-guided systematic (TRUS) biopsy is commonly used in clinical practice to detect clinically significant prostate cancer (PCa)[1-3]. In this study, a more advanced biopsy, MRI-TRUS fusion targeted biopsy, is used together with MRI-derived PI-RADS V2 scoring system for the diagnosis of clinical significant PCa. The values of the two biopsy methods are compared.
Objective
To evaluate the combination of multi-parametric MRI (mpMRI) derived PI-RADS V2 scoring system and MRI-TRUS fusion targeted biopsy in the diagnosis of clinical significant prostate cancer.
Materials and Methods
A prospective analysis was performed in 168 patients with suspected prostate cancer from September 2015 to June 2018. Suspicious areas on mpMRI were defined and graded using PI-RADS score. The T2WI, DWI, ADC data and dynamic contrast enhancment (DCE) quantitative maps were used, and the data acquisition was performed on a 3T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany). All the patients received a transrectal ultrasound-guided systematic (TRUS) biopsy, 108 patients with PI-RADS V2 scores ≥ 3 had additional MRI-TRUS targeted biopsies. The detection rate of TRUS biopsy and suspicious MRI targeted biopsy in PCa and clinical significant cancer were tested by χ2 test on the results of MRI-TRUS fusion guided biopsy.Results
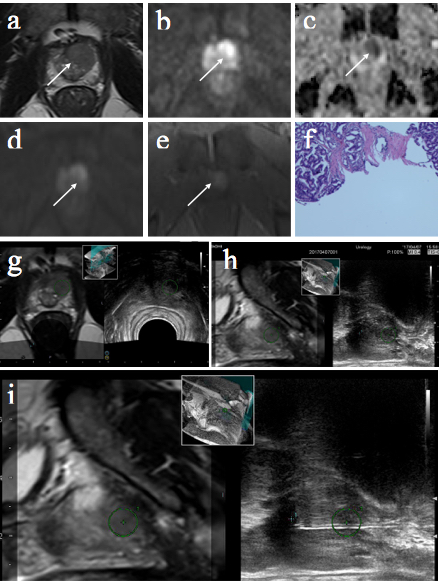
All the 168 patients underwent TRUS biopsy, and 108 patients, whose PI-RADS V2 scores were ≥ 3, had MRI-TRUS fusion guided biopsy to confirm their diagnosis (two examples are shown in Figures 1 & 2). Prostate cancer was detected in 86 of 168 patients (51.19%, 86/168), and no prostate cancer were detected in the rest 82 patients (48.81%,82/168). 78 (46.43%, 78/168) cases of PCa were detected by TRUS biopsy, and 63(58.33%, 63/168) cases of PCa were detected by MRI-TRUS fusion guided biopsy, the difference was statistically significant between TRUS biopsy and MRI-TRUS fusion guided biopsy (χ2=3.73, p=0.035). Further, the 168 patients were biopsied with a total of 2300 cores, including TRUS biopsy 2016 cores and MRI-TRUS fusion targeted biopsy 284 cores. Additionally, the detection rate per core obtained from MRI-TRUS fusion targeted biopsy (51.76%, 147/284) was significantly better than that from TRUS biopsy cores (19.64%, 396/2016;χ2=142.38,p<0.05). Among patients with a positive biopsy for PCa, the number of biopsy cores for conventional TRUS biopsy and MRI-TRUS was 1032 and 214 cores, respectively. The suspicious MRI-TRUS fusion-targeted biopsy (68.69%, 147/214) detected more prostate cancers which had statistical differences compared with TRUS biopsy (38.37%, 396/1032;χ2=66.27, p<0.05). Last but not least, MRI-TRUS fusion targeted biopsy (69.74%, 106/152) showed more significant cancer cores than that of TRUS biopsy (54.50%, 351/644; χ2=11.67, p<0.05).Conclusions
MRI-TRUS fusion targeted biopsy increases the positive rate markedly and improves the detection rate of clinical significant PCa in comparison with TRUS biopsy.Acknowledgements
No acknowledgement found.References
1. Siegel, C., Re: Transition zone prostate cancer: detection and localization with 3-T multiparametric MR imaging. J Urol, 2013. 190(3): p. 881.
2. Weinreb, J.C., J.O. Barentsz, P.L. Choyke, et al, PI-RADS Prostate Imaging - Reporting and Data System: 2015, Version 2. Eur Urol, 2016. 69(1): p. 16-40.
3. Manfredi, M., T.B. Costa Moretti, M. Emberton, et al, MRI/TRUS fusion software-based targeted biopsy: the new standard of care? Minerva Urol Nefrol, 2015. 67(3): p. 233-46.
Figures