1840
The Diagnostic Evaluation of PI-RADS V2 based on Simplified Biparametric MRI for Clinically Significant Prostate CancerJIE BAO1, Xi-ming Wang1, Chun-hong Hu1, and Zhong-shuai Zhang2
1The First Affiliated Hospital of Soochow University, suzhou, China, 2MR Scientific Marketing, Siemens Healthcare, Shanghai, SHANG HAI, China
Synopsis
This study compare the performance of the PI-RADS scores obtained by using biparameter MRI (T2W and diffusion) and multi-parameter MRI (T1W, T2W, diffusion and DCE) for clinically significant PCa, respectively. The results show that the PI-RADS score acquired from biparameter MRI is comparable with that from the traditional multi-parameter MRI.
Propose
This study compare the performance of the PI-RADS scores obtained by using biparameter MRI (bpMRI, including T2W and diffusion) and multi-parameter MRI (mpMRI including T1W, T2W, diffusion and DCE) for clinically significant PCa, respectively. In addition, the consistency of bpMRI based PI-RADS score was also investigated among different radiologists.
Materials and Methods
MpMRI was performed for 333 patients with suspicious lesions on a 3T MR scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany) including high-spatial-resolution structural imaging in several planes, diffusion-weighted imaging and DCE MR imaging. For bpMRI, two radiologists (9 years and 4 years prostate MRI reading experience, respectively) scored only the cross-sectional T2W image and DWI for all cases in strict accordance with the PI-RADS V2 scoring standard without knowing the patient's clinical data and pathology results. Then, Standard PI-RADS V2 scores for all mpMRI was performed after two weeks by the same readers. Interobserver agreement of all PI-RADS V2 scores of two radiologists was investigated. All cases were scored by the author based on mpMRI-based PI-RADS V2 before biopsy. The patients with suspicious tumors PI-RADS V2 assessment category of≥3 were selected for MRI-TRUS targeted biopsy within two weeks after MRI. The other patients with PI-RADS V2 assessment category of 1and 2 were selected for TRUS biopsy. The receiver operating characteristic curves were obtained by PI-RADS V2 scores based on bpMRI and mpMRI sequences, respectively, to record the AUC, accuracy, sensitivity, specificity, positive predictive value and negative predictive value. The diagnostic efficacy of bpMRI and mpMRI for prostate disease was evaluated by MRI-TRUS targeted biopsy and TRUS biopsy.Results
A cohort of 333 patients was performed including 162 PCa (including 150 clinically significant and 12 non-clinically significant PCa) and 171 non-PCa. bpMRI detected PCa in 131 patients and clinically significant PCa in 126 patients; mpMRI detected PCa in 138 patients and clinically significant PCa in 127 patients; Interobserver agreement of bpMRI and the mpMRI of two radiologists was substantial (k = 0.678 and 0.660). The AUC of PI-RADS V2 score based on bpMRI and mpMRI for the diagnosis of benign and malignant prostate lesions was 0.869 and 0.889, respectively, and the difference was not statistically significant (P=0.0638). The accuracy of bpMRI in the diagnosis of benign and malignant prostate diseases is 81.68% (272/333), the sensitivity is 80.86% (131/162), the specificity is 82.46% (141/171), the positive predictive value is 81.37 % (131/161), and the negative predictive value is 81.98 % (141/172). The accuracy of mpMRI score in the diagnosis of benign and malignant prostate lesions was 84.98% (283/333), the sensitivity was 85.18% (138/162), the specificity was 84.80% (145/171), the positive predictive value was 84.15% (138/164) and the predicted value is 85.8% (145/169). The AUC of PI-RADS V2 score based on bpMRI and mpMRI for the diagnosis of clinically significant prostate cancer was 0.879 and 0.890, respectively, and the difference was not statistically significant (P=0.1685). The diagnostic accuracy of bpMRI for clinically significant prostate cancer was 84.38%(281/333), the sensitivity was 92.42%(122/132), the specificity was 79.10%(159/201), the positive predictive value was 74.39%(122/164), and the negative predictive value was 94.08%(159/169); The diagnostic accuracy of mpMRI was 85.59%(285/333), the sensitivity was 93.94% (124/132), the specificity was 80.10% (161/201), the positive predictive value was 75.61% (124/164), and the negative predictive value was 95.27%(161/169).Conclusion
BpMRI can effectively detect clinical significant prostate cancer; the diagnosis performance of bpMRI is similar to that of mpMRI for detecting prostate cancer. As a result, using bpMRI method can significantly shorten the acquisition and interpretation time and avoid the potential risk of DCE injection of contrast agent.Acknowledgements
No acknowledgement found.References
Figures
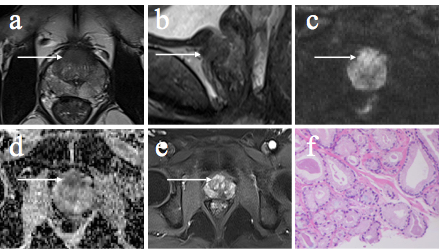
Figure 1. 60 years old male with a prostate-specific antigen (PSA) of 7 ng/ml. Transversal and coronal T2W image (a & b) demonstrate low signal intensity (shown by the arrow). The DWI (c) and ADC (d) show high and low intensity, respectively. e is the dynamic contrast enhanced (DCE) image, which indicates early enhancement. The results of bpMRI and mpMRI are both 5 according to PI-RADS V2. The MR-TRUS targeted biopsy confirmed PCa (f, Gleason score: 3+3 = 6).
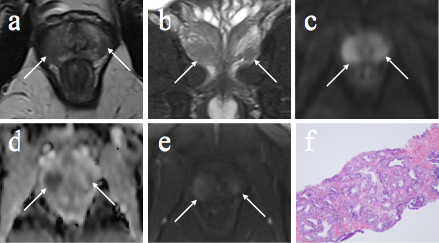
Figure 2. 55 years old male with a PSA of 23.47 ng/ml. Transversal and coronal T2W image (a & b) demonstrate multiple low signal intensity lesions (shown by the arrows). The DWI (c) and ADC (d) show high and low intensity, respectively. e is the dynamic contrast enhanced (DCE) image, which indicates early enhancement. The results of bpMRI and mpMRI are both 5 according to PI-RADS V2. The MR-TRUS targeted biopsy confirmed PCa (f, Gleason score: 4+5 = 9).