1839
Detection of prostate cancer in the peripheral zone using machine learning and multiparametic MRI1The University of Newcastle, Newcastle, Australia, 2Calvary Mater Newcastle, Newcastle, Australia, 3Hunter Medical Research Institute (HMRI), Newcastle, Australia
Synopsis
The aim of this study is to provide a non-invasive voxel based malignant lesion detection tool and probability map for the peripheral zone (PZ) using multi parametric magnetic resonance imaging incorporating DTI as well as standard sequences. A combination of radiomics features extracted from MRI and DTI and supervised machine learning was to develop a tool for cancer detection. Our results demonstrated DTI, when used within the framework of supervised classification, can play a role in the prostate cancer detection. In addition, the posterior probability provide useful information about tumor heterogeneity and may offer better detection of PZ prostate cancer.
Introduction
At present, the ability of non-invasive detection and localization of prostate cancer (PCa) remains challenging (1). Clinical application of magnetic resonance images (MRI) has been shown to improve the detection of prostate cancer. In addition, multi-parametric MRI (mp-MRI), which combines T2-weighted imaging (T2WI), with methods including diffusion-weighted imaging (DWI) and dynamic contrast enhancement (DCE) are utilized clinical management of prostate cancer (2). Mp-MRI using T2WI, DWI and diffusion tensor imaging (DTI) are not currently used for prostate cancer detection. Difficulties in the processing and interpretation of DTI has limited the role of this imaging in the clinic (3). DTI can also yield several other quantitative parameters that to our knowledge have not been evaluated in the detection of prostate cancer. These include axial diffusivity (AD), volume ratio (VR), linear, planar and spherical anisotropy (Cl, Cp and Cs respectively) and so on (4). Therefore incorporation of DTI including these new parameters could improve prostate machine learning systems. In addition, the majority of previous prostate tumour detection systems have performed a binary cancer or no-cancer classification (5). However producing a statistical probability of tumor presence will be a useful tool for the non-invasive assessment of cancer heterogeneity and response to treatment (6).Material and methods
In vivo mp-MRI images were collected from 12 prostate cancer patients (71.16 ± 8.17 years were analysed and three patients were excluded from the study due to motion artefacts. Ethics approval for the study was obtained and written informed consent was obtained from all patients. Participants were scanned using a 3 tesla MRI scanner (Skyra, Siemens Healthineers, Germany) equipped with an phase array coil. T2WI was obtained using a two-dimensional turbo spin echo (TSE). DWI was obtained using single shot echo planar imaging (EPI) and b-values of 0, 400 and 800 s/mm2. DTI was also obtained using a single shot EPI. Thirty non-collinear directions of the diffusion sanitizing gradient were used with a b-values of 0 and 1600 s/mm2. In this study, 192 radiomics features were extracted from each voxel centered within cancer and healthy ROIs on mpMRI images. These quantitative features included 171 features from T2WI, DWI and ADC map (Grey-level features, first order texture feature, second order texture features and gradient based features) and 21 diffusivity and anisotropy features from DTI. Each of the extracted features were normalized to be more sensitive to the classification model using the min-max scale method so that the minimum value is 0 and maximum value is 1. Principal component analysis (PCA) with a 95% confidence interval was used for dimension reduction. Based on features set selected from mp-MRI, six different radial bias function kernel support vector machine (SVM) (RBF-SVM) classifiers were developed and validated using a leave-two-out validation methodology (to avoid overfitting). RBF-SVMs were developed on the train data sets using the reduced features and Bayesian optimization used to find the optimal kernel parameters. The diagnostic performance of each classifier was evaluated using the area under the receiver operating characteristic (ROC) curve. The sensitivity, specificity and accuracy of the models were evaluated using the testing dataset. Finally, the RBF-SVM plus sigmoid combination of the model with the highest performance was used to produce cancer probabilities of the entire peripheral zone for the corresponding test data sets.Results and Discussion
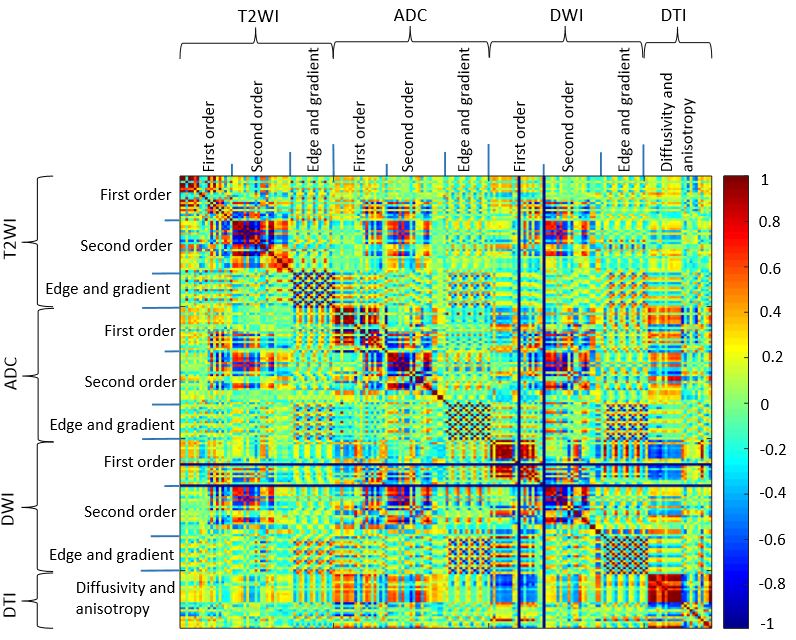
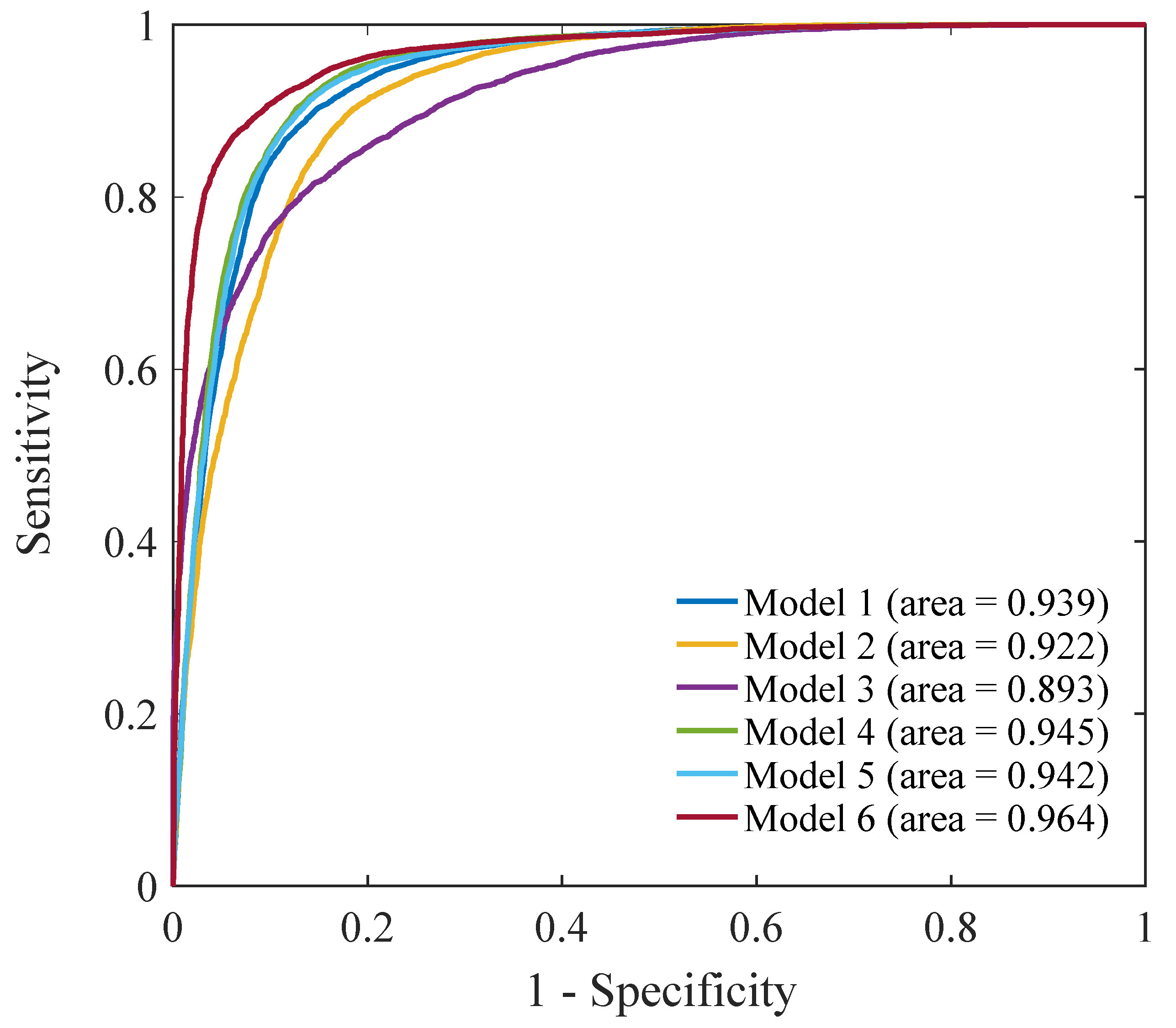
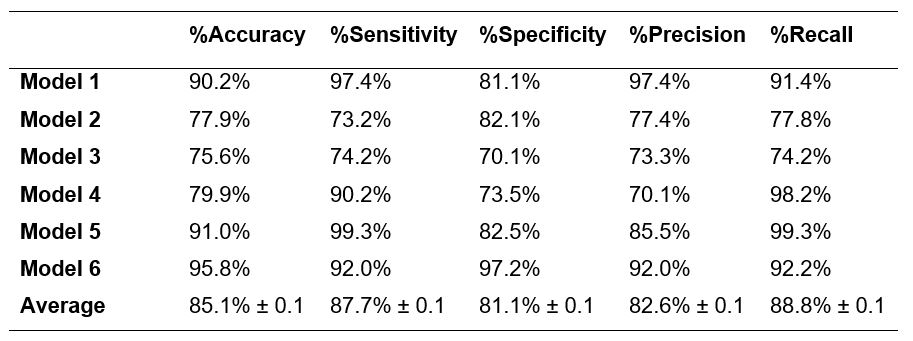
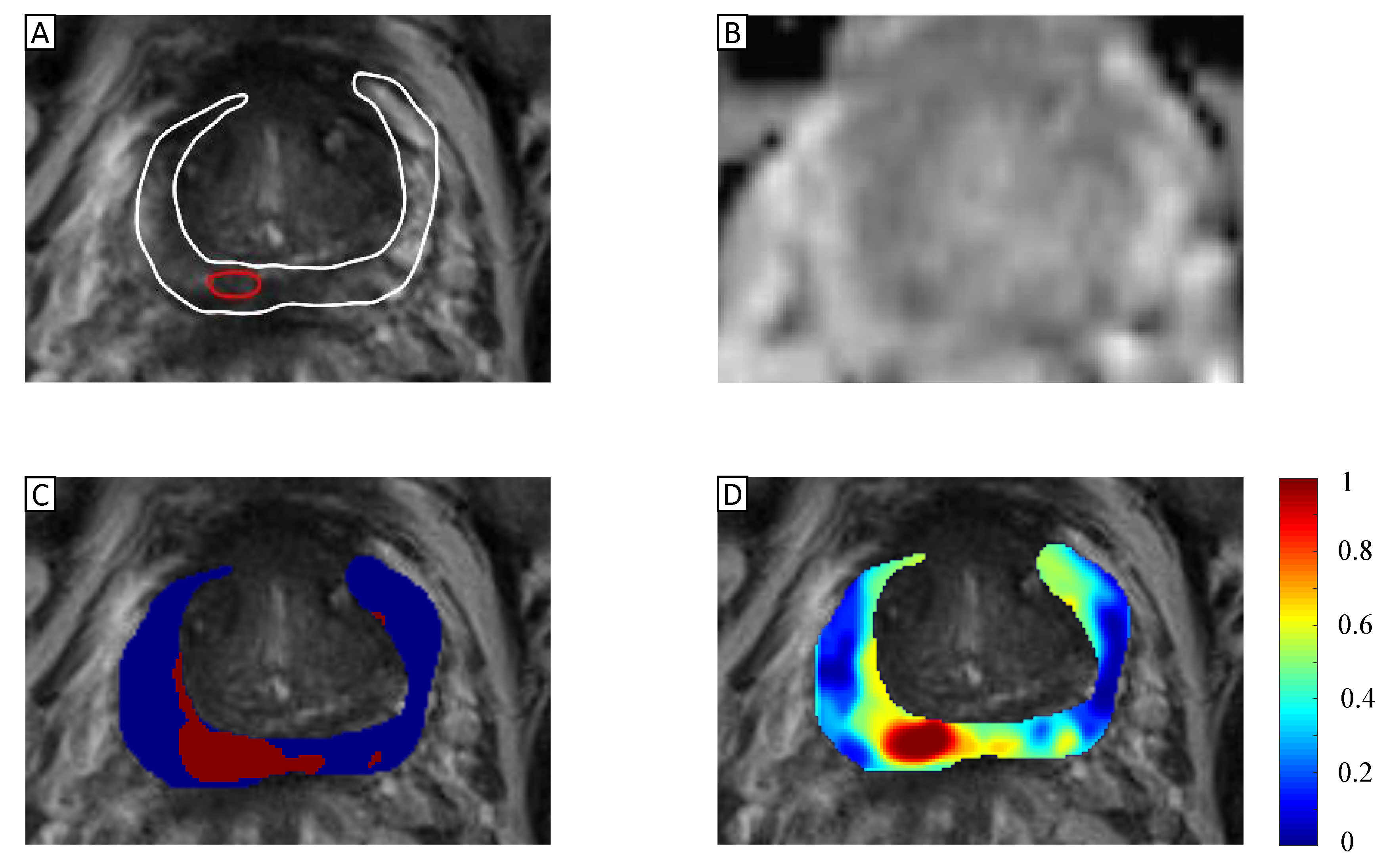
The Pearson correlation heat map of the total extracted features are displayed in Figure 1. The average result of the six optimized RBF-SVM classifiers yielded an area under the ROC curve of 0.934 ± 0.022 (0.893-0.964) for discrimination of cancer and non-cancer voxels (Figure2). The classifiers achieved an average sensitivity of 87.7% ± 0.1 (73.3%-97.4%), specificity of 81.1% ± 0.1 (70.2%-97.3%) and accuracy of 85.1% ± 0.1 (79.9%-95.9%) (Table 1). These results show that machine learning technique with a RBF-SVM and PCA dimension reduction technique can successfully detect prostate cancer in the PZ. Such a diagnostic system tool may allow for faster patient evaluations while helping to increase diagnostic consistency. Figure 3 shows the T2WI, binary output and posterior probability of RBF-SVM classifier for the PZ of the patient data set of the RBF-SVM model with the area under ROC curve of 0.964.Conclusion
A machine learning systems using T2WI, DWI and DTI and Bayesian optimization method are described which are able to differentiate cancer from non-cancer with a high accuracy. The binary output generated by the classifier could help radiologist to find the accurate boundary of cancer in PZ. The addition of a cancer probability model provides additional functionality for image interpretation.Acknowledgements
This research was supported by the Imaging Centre of the University of Newcastle and Calvary Mater Newcastle. We would especially like to acknowledge the contribution of the Clinical Research and Statistical Support unit in Hunter Medical Research Institute (HMRI).References
1. Lemaitre G, Marti R, Freixenet J, Vilanova JC, Walker PM, Meriaudeau F. Computer-Aided Detection and diagnosis for prostate cancer based on mono and multi-parametric MRI: a review. Comput Biol Med 2015;60:8-31.
2.Turkbey B, Choyke PL. PIRADS 2.0: what is new? Diagnostic and Interventional Radiology 2015;21(5):382.
3. Li L, Margolis DJ, Deng M, Cai J, Yuan L, Feng Z, Min X, Hu Z, Hu D, Liu J, Wang L. Correlation of gleason scores with magnetic resonance diffusion tensor imaging in peripheral zone prostate cancer. J Magn Reson Imaging 2015;42(2):460-467.
4. Van Hecke W, Emsell L, Sunaert S. Diffusion Tensor Imaging : a Practical Handbook. 2016.
5. Niaf E, Rouvière O, Mège-Lechevallier F, Bratan F, Lartizien C. Computer-aided diagnosis of prostate cancer in the peripheral zone using multiparametric MRI. Physics in medicine and biology 2012;57(12):3833.
6. Platt J. Probabilistic outputs for support vector machines and comparisons to regularized likelihood methods. Advances in large margin classifiers 1999;10(3):61-74.
Figures