1833
MRI-Derived Patient Specific Molds for Cancer Lesion Analysis in the Prostate1Mechanical Engineering, University of Wisconsin-Madison, Madison, WI, United States, 2Radiology, University of Wisconsin-Madison, Madison, WI, United States, 3Biomedical Engineering, University of Wisconsin-Madison, Madison, WI, United States, 4Pathology, University of Wisconsin-Madison, Madison, WI, United States, 5Urology, University of Wisconsin-Madison, Madison, WI, United States, 6Medicine, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
Magnetic Resonance Imaging (MRI), and emerging Prostate Specific Membrane Antigen (PSMA) Positron Emission Tomography (PET)/MRI, can be used to detect and locate prostate cancer. The accuracy of this method can be validated by comparing post-prostatectomy histopathology information to MRI and PET image data with the help of a custom prostate-sectioning device. This study is aimed at addressing sectioning device limitations proposed by previous studies and at developing a three-dimensional (3D) comparison method for MRI data and post-prostatectomy prostate geometries.
INTRODUCTION
Prostate cancer, one of the most common forms of cancer in America, affects nearly 165,000 men and leads to about 29,000 deaths annually.(1) Magnetic resonance imaging (MRI) has been successful at detecting prostate cancer and locating cancer lesions. However, the spatial accuracy of MR prostate images must still be validated, and appropriate correlation between MRI and histopathology should be made to display the clinical utility of MRI in prostate cancer diagnosis and treatment. Past studies have addressed this problem through the use of MRI-based prostate cutting devices that allow correlation between MRI data and histopathology data from excised prostates.(2-7) The purpose of this study was to address some limitations presented by previous studies and develop a method for 3D comparison between pre-prostatectomy MRI data and post-prostatectomy histological slices.
METHODS
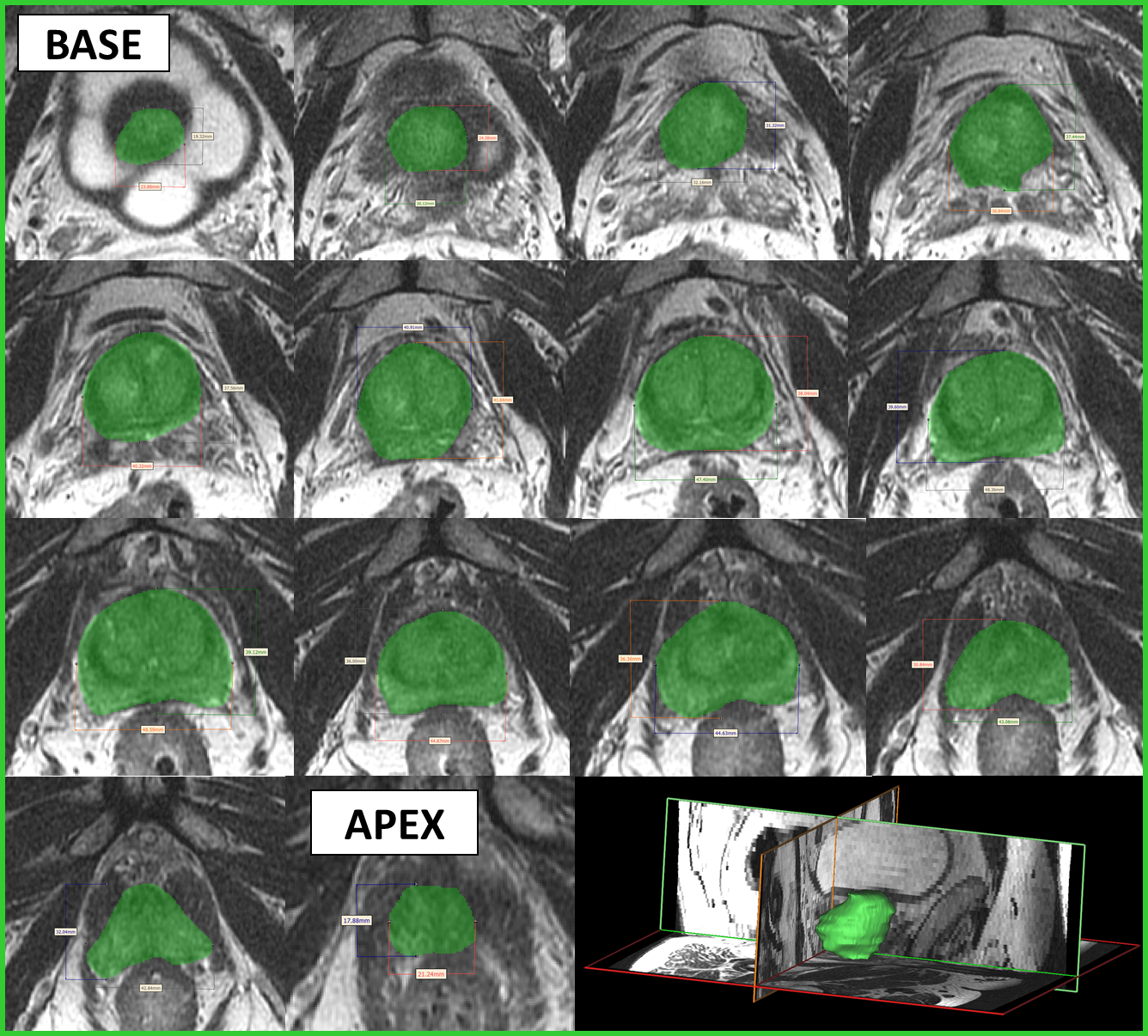
Prostate Specific Membrane Antigen (PSMA) Positron Emission Tomography (PET)/MRI was performed on 13 patients with prostate cancer, both before and after chemohormonal treatment, with an imaging slice thickness of 2.5mm. The post-treatment images were imported into MIMICS (Materialise, Leuven, Belgium), where the boundary of the prostate was contoured under the guidance of an experienced radiologist (Figure 1). The prostate dimensions were measured on each MR image slice and saved for later pathological investigation. The prostate surface was then interpolated between MR image slices and a 3D volume was generated. A 3D model of the prostate was exported into 3-matic design software (Materialise, Leuven, Belgium).
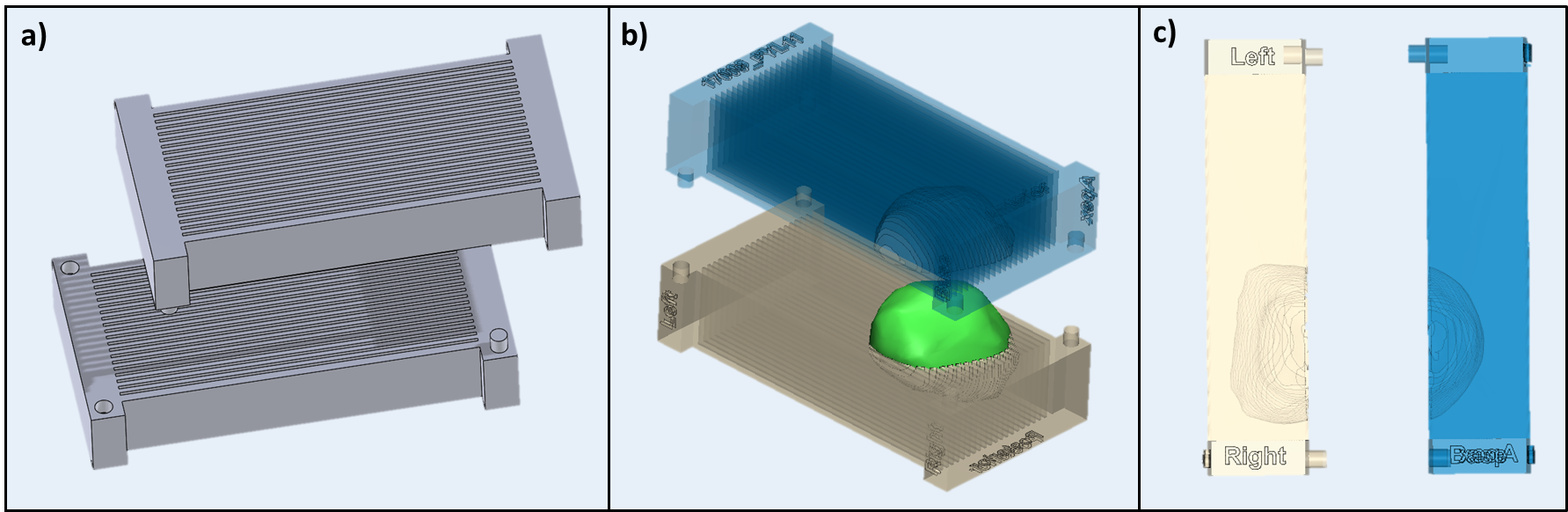
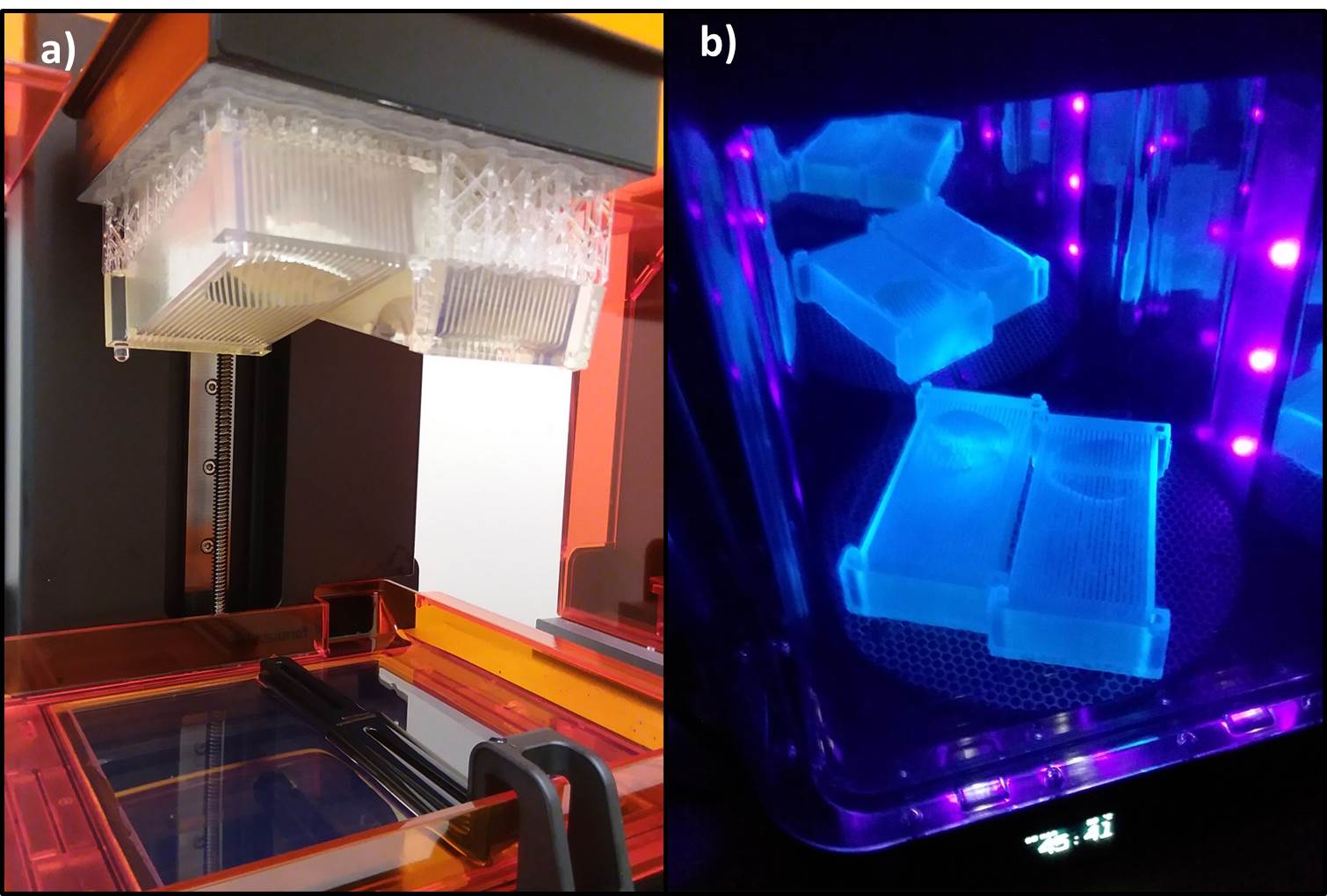
To create a device that allows for consistent cutting of the prostate at 2.5mm increments, a mold template was designed in Solidworks (Dassault Systèmes, Waltham, MA), as shown in Figure 2a. The patient specific prostate surface was subtracted from the mold template volume (Figure 2b). The mold was labeled with the patient study number and anterior/posterior, right/left, and base/apex notations (Figure 2c). The model was then exported to a steriolothography 3D printer (Form2, Formlabs, Somerville, MA). When the print was finished, it was cleaned, sterilized, and cured in isopropyl alcohol and UV light (Figure 3 a&b).
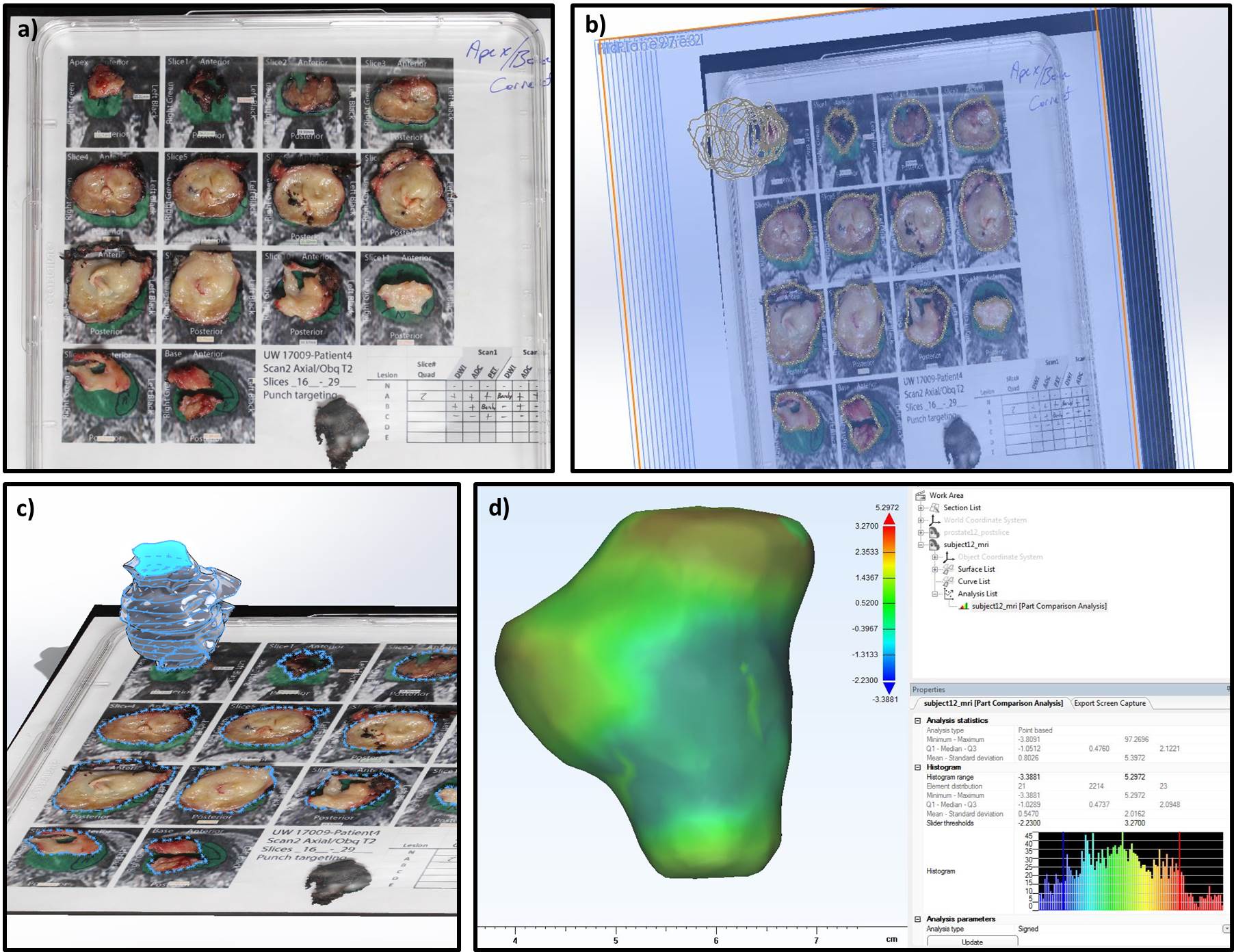
The mold was taken to surgical pathology, where it was used to section the prostate following prostatectomy with a tissue slicer blade (Thomas Scientific). The slices of prostate were then oriented on the MRI-derived 2D contours, as shown in figure4a, and a picture was taken for later analysis. The prostate slices were then taken for histological analysis.
To analyze the 3D accuracy of the MRI-based prostate mold, the post-resection prostate volume was reconstructed based on the prostate slices from surgical pathology. To do this, contours of the prostate slices were stacked on planes 2.5mm apart (Figure 2b), and lofted to create a 3D volume in Solidworks (Figure 4c). A part comparison analysis was then performed in 3-matic to generate regional difference maps comparing the MRI-derived prostate geometry with the representative post-prostatectomy geometry (Figure 4d).
RESULTS
The patient-specific molds were used to effectively slice the unfixed prostate at 2.5mm increments (Figure 4a). This was performed on the same day as prostatectomy before prostate tissue fixation, enabling the dissection of viable portions of tumor for research without reducing the number slices used for pathologic diagnosis. Quality and function of the molds improved with each iteration, and design standards were developed as a result of the post-prostatectomy analysis.DISCUSSION
Pre-prostatectomy MRI data can be compared with post-prostatectomy histopathological prostate slices to determine the utility of MRI for prostate cancer detection and location. This study looked to build upon other studies focused on comparing prostate partitioning and MRI to histology. It has been noted that the fit of the mold to the resected prostate, the slicing technique, and the thickness of the image slices are major factors that affect image-based model performance.(3) Accordingly, this study employed patient-specific molds based upon individualized prostate contours, image slice thickness of 2.5mm (vs 3-6mm used in previous studies) that matched pathology slice thickness, and cutting of unfixed prostate on the day of surgery to evaluate masking of the MRI image and geometric ex-vivo changes to the shape of the prostate.CONCLUSION
A process to create and validate patient-specific MRI-based molds for prostate analysis is proposed. Through the remainder of this study, more quantitative comparison will be performed to analyze the effectiveness of these devices for histopathological prostate analysis with MRI and PET/MRI.Acknowledgements
The research presented was supported by the NIH (UL1TR000427, TL1TR000429) and DOD IMPACT award PC15053. The authors also wish to acknowledge support from GE Healthcare who provides research support to the University of Wisconsin.References
1. Prostate Cancer Facts. Prostate Cancer Foundation; 2018.
2. Drew B, Jones EC, Reinsberg S, Yung AC, Goldenberg SL, Kozlowski P. Device for sectioning prostatectomy specimens to facilitate comparison between histology and in vivo MRI. J Magn Reson Imaging 2010;32(4):992-996.
3. Shah V, Pohida T, Turkbey B, et al. A method for correlating in vivo prostate magnetic resonance imaging and histopathology using individualized magnetic resonance-based molds. Rev Sci Instrum 2009;80(10):104301.
4. Jackson AS, Reinsberg SA, Sohaib SA, et al. Dynamic contrast-enhanced MRI for prostate cancer localization. Br J Radiol 2009;82(974):148-156.
5. Kimm SY, Tarin TV, Lee JH, et al. Methods for registration of magnetic resonance images of ex vivo prostate specimens with histology. J Magn Reson Imaging 2012;36(1):206-212.
6. Yamamoto H, Nir D, Vyas L, et al. A Workflow to Improve the Alignment of Prostate Imaging with Whole-mount Histopathology. Acad Radiol 2014;21(8):1009-1019.
7. Hughes C, Rouvière O, Mege-Lechevallier F, Souchon R, Prost R. Robust alignment of prostate histology slices with quantified accuracy. IEEE Trans Biomed Eng 2013;60(2):281-291.
Figures