1830
Improving prostate cancer detection in mp-MRI via CNN using the joint loss1Radiology, University of California, Los Angeles, Los Angeles, CA, United States, 2Computer Science, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
We proposed an improved CNN using joint loss to fully utilize multi-parametric imaging for the automated prostate cancer detection in mp-MRI. 397 pre-operative mp-MRI exams were collected in our medical center, and lesion ROIs were retrospectively annotated with whole-mount histopathology confirmations. The improved CNN achieved 75.1% detection sensitivity at 1 false positive per patient and had an AUC 0.901 in the ROC analysis.
Introduction
Multi-parametric MRI (mp-MRI) is a powerful imaging tool for the diagnosis of prostate cancer (PCa). However, its diagnostic utility is limited by the current interpretation of mp-MRI, based on qualitative and semi-quantitative assessments, causing inter-reader variability1. Here, we propose an improved convolutional neural network (CNN) to automatically detect PCa using mp-MRI. The improved CNN is trained and tested using the joint loss of focal loss and mutual finding loss, specifically designed for mp-MRI, with 546 annotated PCa lesions.
Materials and Methods
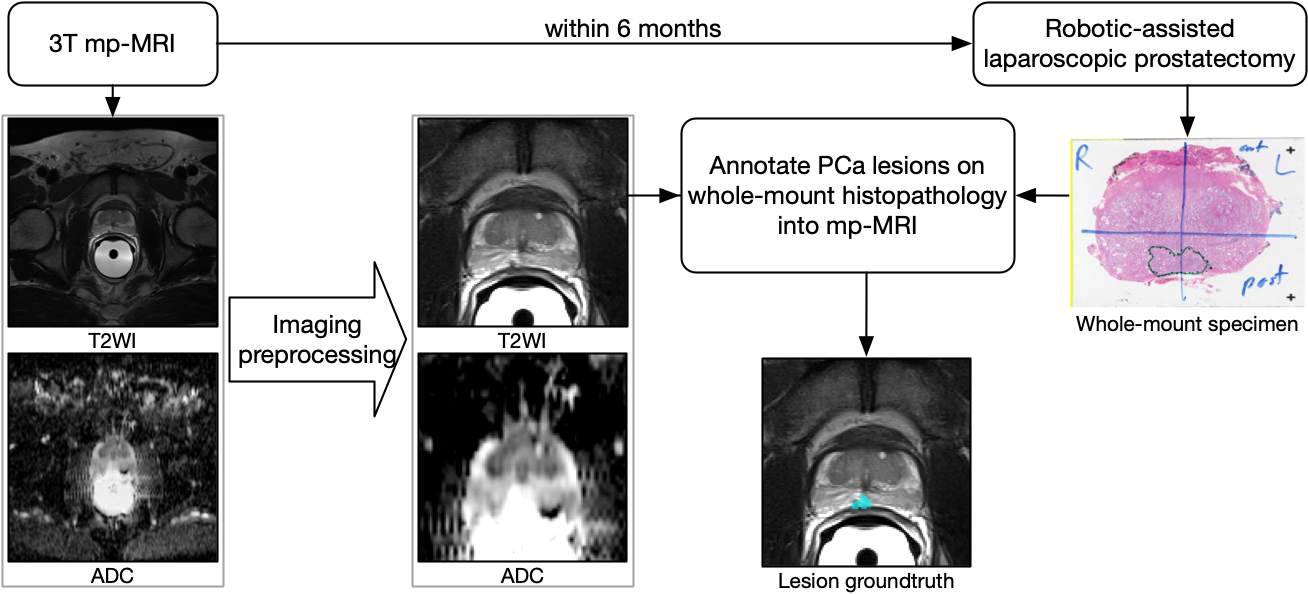
With IRB approval, we retrospectively collected 397 pre-operative mp-MRI exams from patients whom 1) opted to robotic-assisted laparoscopic prostatectomy (RALP), 2) had at least one lesion with Gleason score>6 or diameter≥10mm, and 3) did not undergo radiotherapy or hormonal therapy prior to RALP. mp-MRI exams were acquired using the standard clinical protocol in one of three different 3T scanners (Trio, Skyra, Prisma; Siemens Healthcare). T2-weighted imaging (T2WI) and diffusion-weighted imaging (DWI) were acquired, and T2WI and maps of apparent diffusion coefficient (ADC) were used in this study. The PCa regions of interest (ROIs) were identified and annotated in mp-MRI using the whole-mount histopathology as a reference. PCa lesions with GS=6 and diameter<10mm were excluded due to their limited visibility in mp-MRI2. In this study cohort, 546 lesions were annotated, including 112 GS=6 lesions, 266 GS 3+4 lesions, 109 GS 4+3 lesions, and 59 GS≥8 lesions.
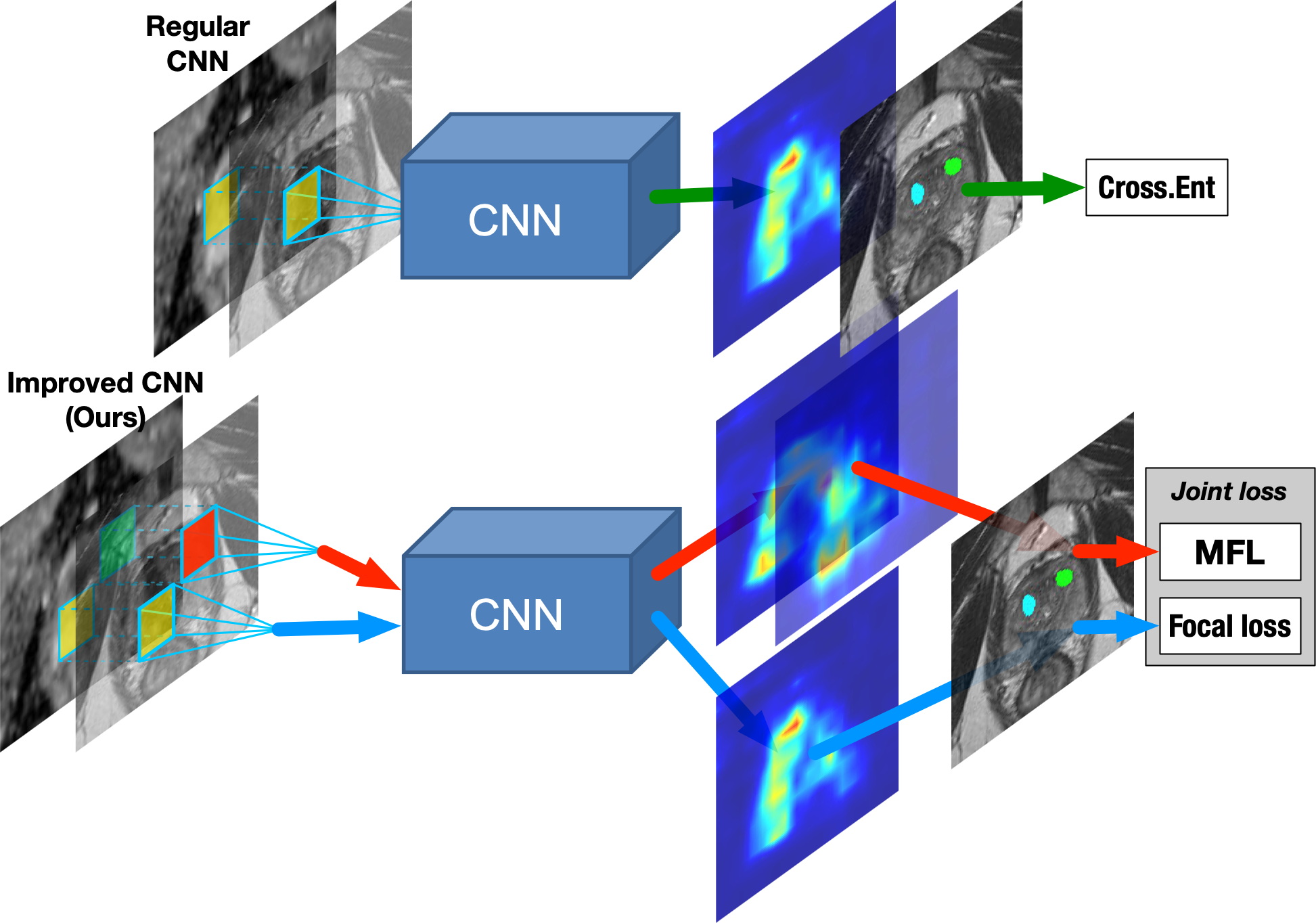
We built a 101-layer deep residual network with atrous convolutional filters3 to segment PCa lesions in pixel-level in mp-MRI. The corresponding T2WI and ADC are stacked together as two channels of the CNN input for each slice, and the annotated lesion mask serves as the groundtruth during the end-to-end training. The CNN is trained by the joint loss of focal loss and mutual finding loss. Focal loss4 is a variant of the cross-entropy loss defined as
$$\left(1-p\right)^2y\log\left( p\right)+p^2\left(1-y\right)\log\left(1-p\right),$$
where $$$p$$$ is the predicted lesion probability and $$$y$$$ is the binary label. Focal loss balances the loss from cancerous and non-cancerous pixels. Moreover, we designed mutual finding loss (MFL) to train with respect to a subset of imaging components in mp-MRI, as in Figure 2. Given the CNN, $$$f$$$, with $$$I_\mathrm{ADC}$$$ and $$$I_\mathrm{T2WI}$$$ stacked as the input, MFL is defined as
$$\min\{dist\left(f\left(I_\mathrm{ADC},\cdot\right)-f_\mathrm{out}\right),dist\left(f\left(\cdot,I_\mathrm{T2WI}\right)-f_\mathrm{out}\right)\}$$
where $$$f_\mathrm{out}= f\left(I_\mathrm{ADC},I_\mathrm{T2WI}\right)$$$ and $$$dist$$$ is the L2-distance. MFL compares whether $$$I_\mathrm{ADC}$$$ or $$$I_\mathrm{T2WI}$$$ alone can produce output more similar to $$$f_\mathrm{out}$$$ as the truth reference on lesion regions. During the training, MFL minimizes the difference between the output using a single imaging component alone and the output with both components.
The intensity of T2WI is normalized based on the intensity of bladder for each case, as we find bladder easy to be localized, and the intensity is relatively consistent across patients. During testing, the lesion detection points are proposed by searching for local minimums from the pixel-level lesion prediction output of the slices from each case.
Results
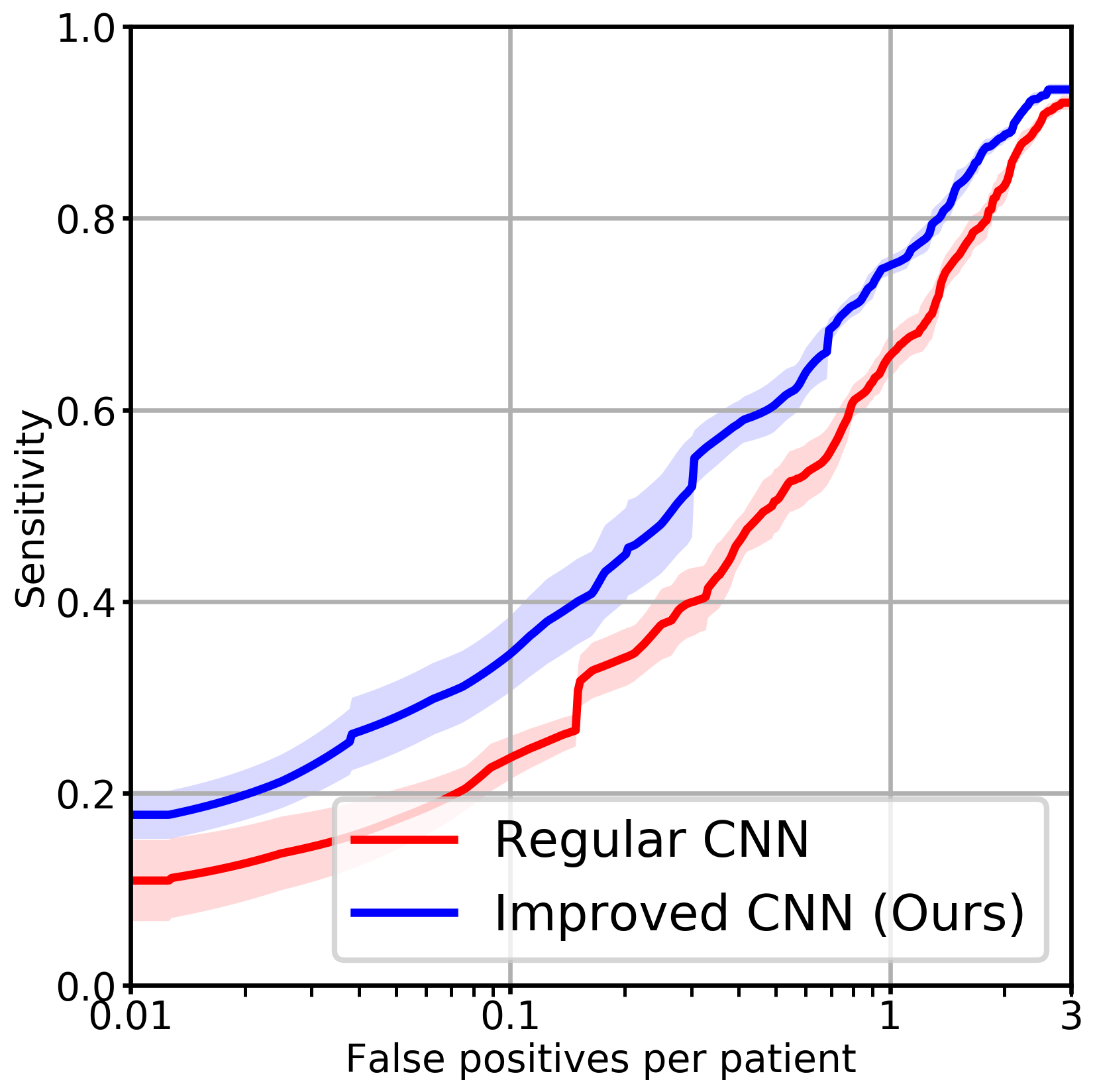
The improved CNN using the joint loss and a baseline CNN using the cross-entropy loss (with the same network architecture) were trained and validated in 5-fold cross-validation. Each fold contained 313 or 314 cases for training and the remaining for testing. In the evaluation, the detection points were considered true positives if in or within 5mm of the annotated lesion contours, or false positives if otherwise. The free-response receiver operating characteristic (FROC) analysis5 measured the lesion detection sensitivity versus the number of false positive detection per patient on average. In Figure 4, our improved CNN trained by the joint loss achieved 75.1% lesion detection sensitivity at 1 false positive per patient, improving 9.4% from the baseline CNN.
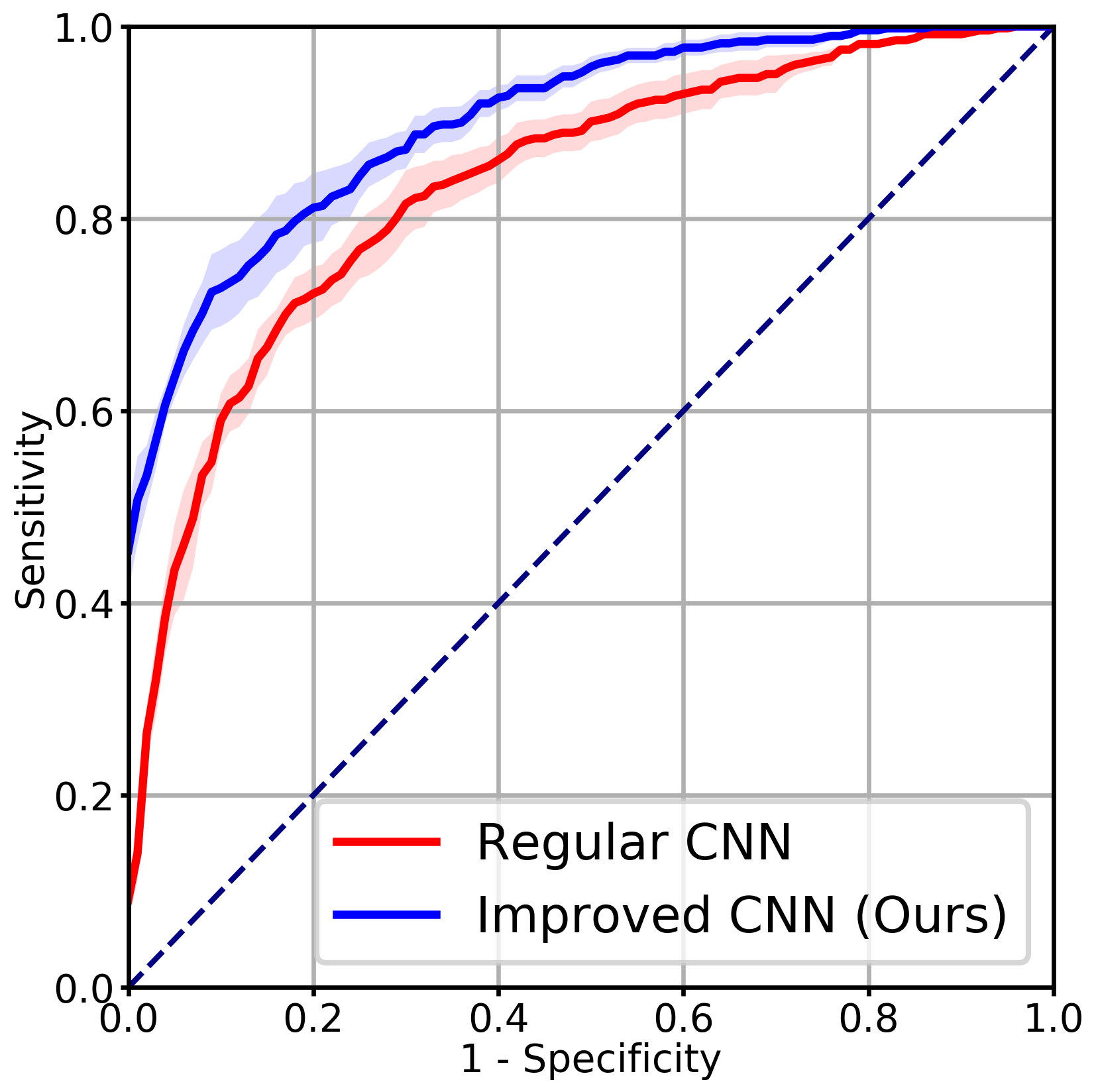
We also evaluated lesion detection using receiver operating characteristic (ROC) analysis6. The annotated lesions were positive ROIs, and the negative ROIs were obtained by taking the horizontal symmetry of the positive ROIs. The average prediction probability for each ROI was used as the prediction value to the ROC. As in Figure 5, while the baseline CNN received the area under the curve (AUC) 0.835±0.017, our model had an AUC 0.901±0.011, which was significantly higher (p<0.02).
Discussion and Conclusion
While we only showed the joint loss using two imaging components, MFL can be extended to more components with the cost of additional GPU memory consumption and computational overhead.
In conclusion, we improved the CNN using the joint loss to fully account for multi-parametric imaging for prostate cancer detection in mp-MRI. The proposed CNN with the joint loss improved the detection sensitivity by 9.4% from the baseline CNN at 1 false positive per patient in FROC analysis and achieved an AUC 0.901 in the ROC analysis.
Acknowledgements
This work was supported by funds from the Integrated Diagnostics Program, Department of Radiological Sciences & Pathology, David Geffen School of Medicine at UCLA.References
1. Ruprecht, Oliver, et al. "MRI of the prostate: interobserver agreement compared with histopathologic outcome after radical prostatectomy." European journal of radiology 81.3 (2012): 456-460.
2. Tan, Nelly, et al. "Characteristics of detected and missed prostate cancer foci on 3-T multiparametric MRI using an endorectal coil correlated with whole-mount thin-section histopathology." American Journal of Roentgenology 205.1 (2015): W87-W92.
3. Chen, Liang-Chieh, et al. "Deeplab: Semantic image segmentation with deep convolutional nets, atrous convolution, and fully connected crfs." IEEE transactions on pattern analysis and machine intelligence 40.4 (2018): 834-848.
4. Lin, Tsung-Yi, et al. "Focal loss for dense object detection." IEEE transactions on pattern analysis and machine intelligence (2018).
5. Litjens, Geert, et al. "Computer-aided detection of prostate cancer in MRI." IEEE transactions on medical imaging 33.5 (2014): 1083-1092.
6. Song, Yang, et al. "Computer‐aided diagnosis of prostate cancer using a deep convolutional neural network from multiparametric MRI." Journal of Magnetic Resonance Imaging (2018).
Figures