1826
Preoperative Differentiation of Uterine Sarcoma from Leiomyoma: Comparison of Three Models Based on Different Segmentation Volumes Using RadiomicsHuihui Xie1, Xiaodong Zhang1, and Xiaoying Wang2
1Department of Radiology, Peking University First Hospital, BEIJING, China, 2Peking University First Hospital, BEIJING, China
Synopsis
This study aimed to explore that if the segmentation of different volume
of interests (VOIs) may influence the diagnostic performance of radiomic model.
We included 78 patients with pathologically confirmed uterine sarcomas or
atypical leiomyomas. 3 different VOIs were manually drawn on images of ADC maps.
Radiomic models were built based on three feature set. Features extracted from VOI
covered the whole uterus had the best diagnostic performance than VOI covered
the lesion or lesion and some surrounded tissue. It suggested VOI covered the whole uterus added relevant information for distinguishing
uterine sarcoma from atypical leiomyoma.
Introduction
Radiomic involves extraction and modeling of a large number of medical imaging features for diagnostic, prognostic, and predictive purpose. Segmentation of VOI is the most important way in radiomic analysis. It determines which voxels within an image are analyzed. In conventional image interpretation, the differentiation of uterine sarcoma and leiomyoma in magnetic resonance imaging (MRI) depends on peri-tumor appearance such as continuity of uterine endometrial cavity, peri-tumor flow voids, ill-defined tumor margin as well as intratumor characteristics such as intratumor hemorrhage or necrosis. VOI contains tumor region alone may left essential voxels outside the region unanalyzed. We hypotheses that if more useful information (defined by conventional image interpretation) can be extracted from VOI and analyzed, the diagnostic performance of radiomic model may improve. The primary objective of this study was to compare the diagnostic performance of radiomic models based on features extracted from three different VOIs in the differentiation of uterine sarcoma and atypical leiomyoma.Methods
78 patients (29 uterine sarcomas, 49 atypical leiomyomas) imaged with pelvic magnetic resonance imaging (MRI) prior to surgery were included in this retrospective study. Manually segmentations of VOIs covered three different regions on apparent diffusion coefficient (ADC) maps: (1) tumor, (2) tumor and some surrounded tissue, and (3) whole uterus (Fig.1). Texture and non-texture features were extracted from each VOI (Fig.2). multivariate models were constructed for each initial feature set and modeled outcome using imbalanced-adjusted logistic regression. The 0.623 + bootstrap method and the area under the receiver-operating characteristic curve (AUC) were used to select the features. 20 logistic regression models (orders of 1–20) based on different combination of image features were built for each way of image segmentation (Fig.3). Finally, the prediction performance of the 3 chosen texture models was estimated using average AUCs, sensitivities, and specificities obtained in 100 bootstrap testing samples.Results
For the first VOI region, model 18 with 18 features yielded the highest AUC of 0.830, sensitivity of 76.0%, specificity of 73.2%, and accuracy of 73.9%. The optimal feature set included 2 histogram-based texture features (Variance, Kurtosis) and 16 high-order texture features (Gray-Level Non-uniformity, Zone-Size Non-uniformity, Complexity, Entropy, Contrast, Correlation, Homogeneity, Energy, Variance, and Dissimilarity). For the second VOI region, model 17 with 17 features yielded the highest AUC of 0.853, sensitivity of 75.5%, specificity of 75.5%, and accuracy of 76.8%. The optimal feature set included 1 non-texture feature (Eccentricity), 3 histogram-based texture features (Skewness), and 13 high-order texture features (Gray-Level Non-uniformity, Run-Length Variance, Short Run Low Gray-Level Emphasis, Long Run Low Gray-Level Emphasis, Long Run High Gray-Level Emphasis, High Gray-Level Run Emphasis, Low Gray-Level Run Emphasis, Low Gray-Level Zone Emphasis, Small Zone High Gray-Level Emphasis). For the third VOI region, model 20 with 20 features yielded the highest AUC of 0.876, sensitivity of 76.3%, specificity of 84.5%, and accuracy of 82.4%. The optimal feature set included 1 non-texture feature (Solidity), 1 histogram-based texture features (Variance), and 19 textural features (Gray-Level Non-uniformity, Zone-Size Variance, Energy, Variance, Entropy, Contrast) (Fig.4). The probability of observing uterine sarcoma as a function of the response of the multivariable models proposed in this work was calculated for all patients of the cohort (Fig. 4)Discussion
VOI covered tumor or subregions only cannot included the whole features caused by tumor’s behavior. With the enlargement of VOI, the sensitivity, specificity, accuracy and AUC raised, especially the specificity. The diagnostic performance of optimal model based on features extracted from VOI No.3 (whole uterus) was the best. Our explanation was that this segmentation method not only covered the features of tumor region but also included the other predictive features outside of the tumor (e.g., ill-defined tumor margin, the interrupted uterine endometrial cavity). It suggested that if we knew how the neural techniques performed, our knowledge of traditional image interpretation may be of use in improving the performance of neural techniques. These introduced a new method of image segmentation that could be of use in the future. However, validation is needed in future studies in other institutions and other diseases. Though optimal features extracted from three different VOIs varied, they all suggested that uterine sarcoma was more heterogenous than atypical leiomyoma. It also illustrated that radiomic analysis had the potential to serve as a noninvasive technique for accurate characterization of tumor microenvironment, thus improving diagnosis. Conclusion Radiomic model based on features extracted from VOI covered the whole uterus had the best diagnostic performance. Adopting VOI contained more useful image information was able to improve diagnostic performance of radiomic model.Acknowledgements
No acknowledgement found.References
1. Lambin P, Rios-Velazquez E, Leijenaar R, et al. (2012) Radiomics: extracting more information from medical images using advanced feature analysis. European journal of cancer 48:441-446. 2. Lambin P, Leijenaar RTH, Deist TM, et al. (2017) Radiomics: the bridge between medical imaging and personalized medicine. Nature reviews Clinical oncology 14:749-762. 3. Gillies RJ, Kinahan PE, Hricak H (2016) Radiomics: Images Are More than Pictures, They Are Data. Radiology 278:563-577. 4. Gevaert O, Mitchell LA, Achrol AS, et al. (2014) Glioblastoma multiforme: exploratory radiogenomic analysis by using quantitative image features. Radiology 273:168-174. 5. Prasanna P, Patel J, Partovi S, Madabhushi A, Tiwari P (2017) Radiomic features from the peritumoral brain parenchyma on treatment-naive multi-parametric MR imaging predict long versus short-term survival in glioblastoma multiforme: Preliminary findings. European radiology 27:4188-4197. 6. Shen C, Liu Z, Guan M, et al. (2017) 2D and 3D CT Radiomics Features Prognostic Performance Comparison in Non-Small Cell Lung Cancer. Translational oncology 10:886-894. 7. Li H, Zhu Y, Burnside ES, et al. (2016) MR Imaging Radiomics Signatures for Predicting the Risk of Breast Cancer Recurrence as Given by Research Versions of MammaPrint, Oncotype DX, and PAM50 Gene Assays. Radiology 281:382-391. 8. Wibmer A, Hricak H, Gondo T, et al. (2015) Haralick texture analysis of prostate MRI: utility for differentiating non-cancerous prostate from prostate cancer and differentiating prostate cancers with different Gleason scores. European radiology 25:2840-2850. 9. Gadducci A, Cosio S, Romanini A, Genazzani AR (2008) The management of patients with uterine sarcoma: a debated clinical challenge. Critical reviews in oncology/hematology 65:129-142. 10. Amant F, Coosemans A, Debiec-Rychter M, Timmerman D, Vergote I (2009) Clinical management of uterine sarcomas. The Lancet Oncology 10:1188-1198. 11. Pietzner K, Buttmann-Schweiger N, Sehouli J, Kraywinkel K (2018) Incidence Patterns and Survival of Gynecological Sarcoma in Germany: Analysis of Population-Based Cancer Registry Data on 1066 Women. International journal of gynecological cancer : official journal of the International Gynecological Cancer Society 28:134-138. 12. Owen C, Armstrong AY (2015) Clinical management of leiomyoma. Obstetrics & Gynecology Clinics of North America 42:67-85. 13. Kim TH, Kim JW, Kim SY, Kim SH, Cho JY (2018) What MRI features suspect malignant pure mesenchymal uterine tumors rather than uterine leiomyoma with cystic degeneration? Journal of gynecologic oncology.Figures
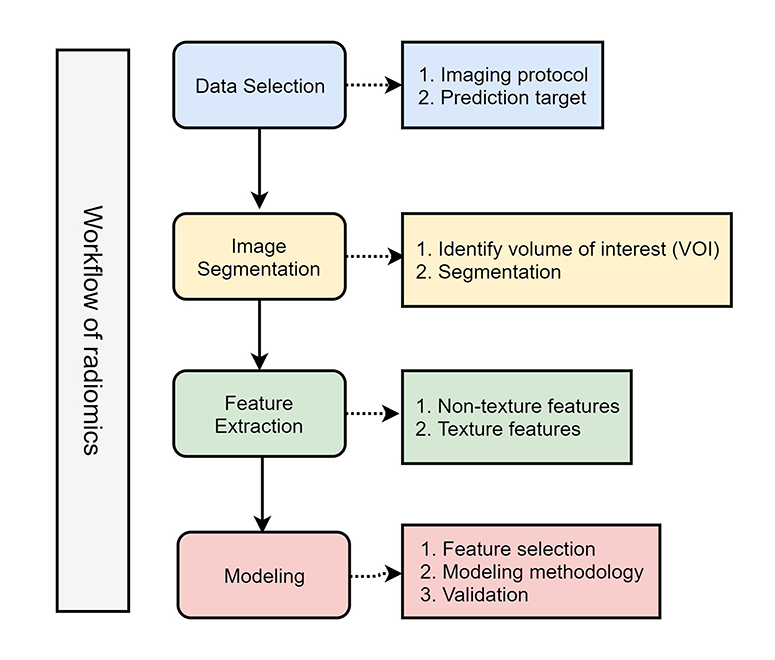
Workflow of radiomics
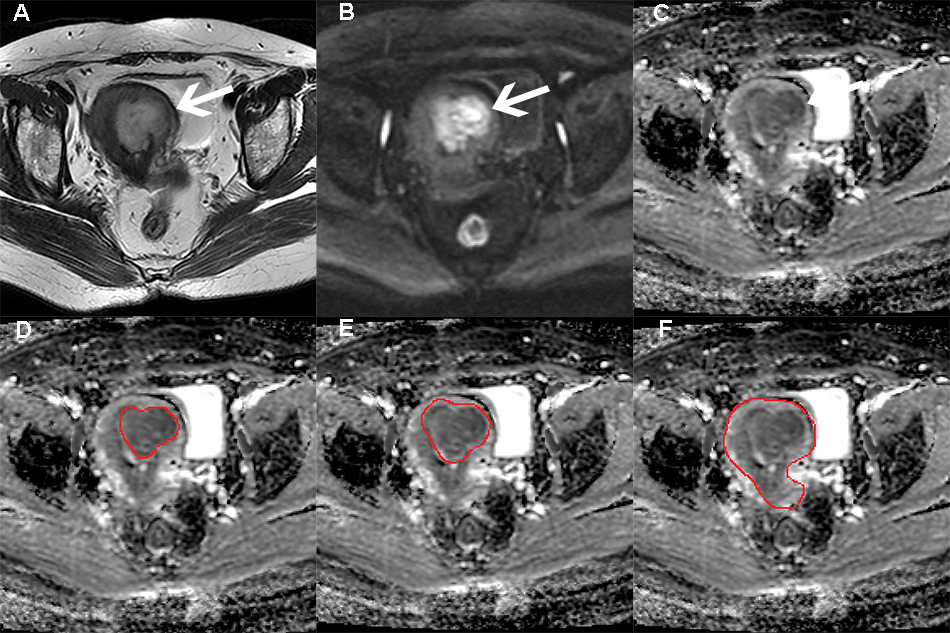
Example of a 58-year old patient with leiomyosarcoma shows image segmentation on ADC maps. Axial T2-weighted
images (A) and DWI (B) show a mass in myometrium (white arrow). C shows a
hypodense mass on ADC maps. D-F show the region of VOI on ADC maps: covered
only the lesion (D), covered the lesion and surrounded tissue (E), and covered
the whole uterus (F).
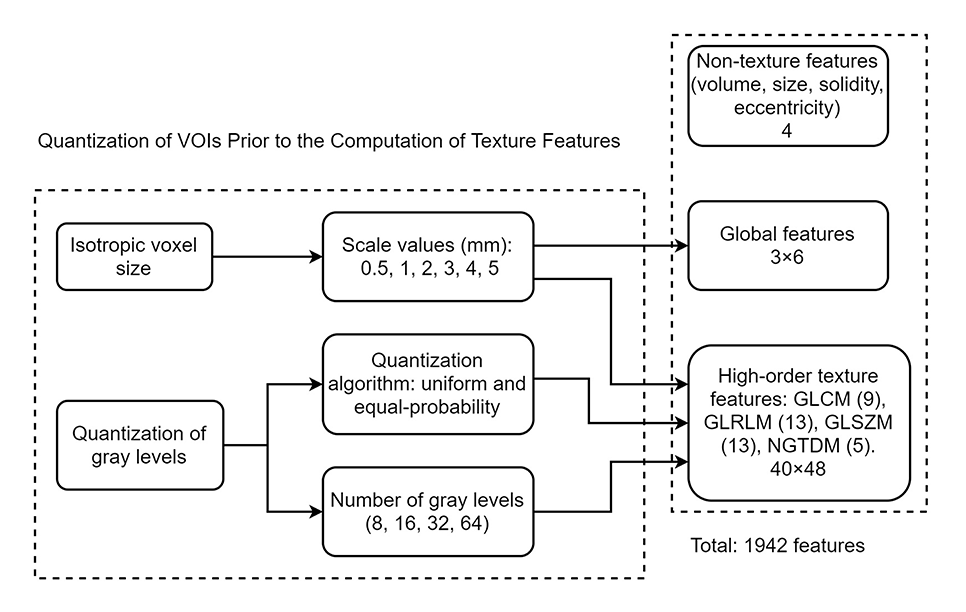
Workflow of radiomic features’ extraction for each VOI.
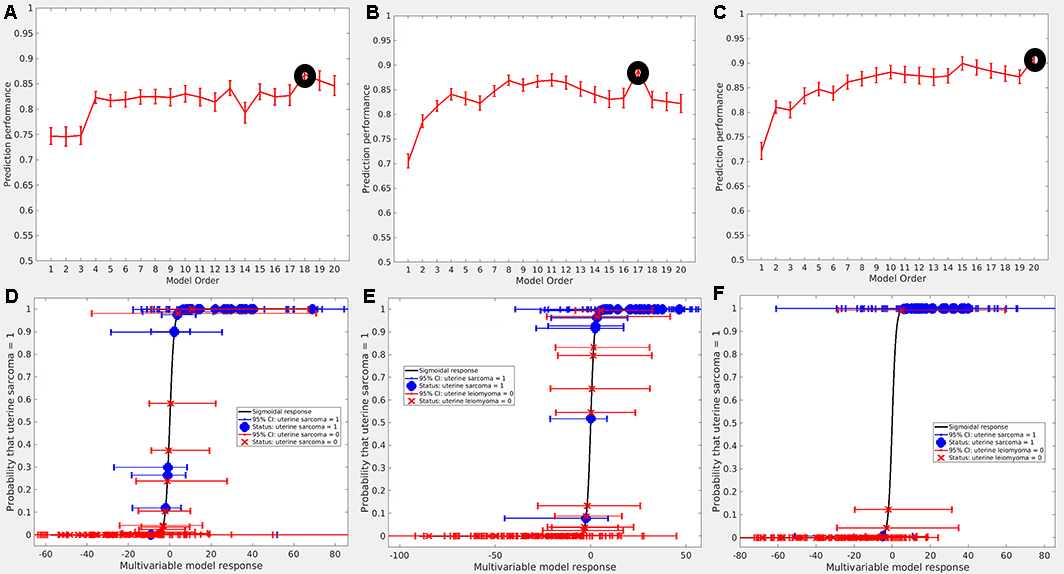
Inspection
of predictive properties of multivariable texture models constructed from 3
feature sets (A-C). Probability of developing uterine sarcoma as a function of
the response of the multivariable model proposed in this work, for all patients
of the cohort (D-F). The dots represent patients who had uterine sarcoma and
the crosses those who had uterine leiomyoma. It can be seen that the optimal
feature models can significantly separate the patients of the 2 pathological
results for each VOI, especially in the case of VOI No. 3.