1825
Comparative Study of DCE-MRI Pharmaceutical Kinetic Models and MVD for Characterizing Endometrial Carcinoma MicrocirculationZhijun Ye1 and Gang Ning1
1West China Second University Hosptial, Chengdu, China
Synopsis
Using five models of DCE MRI and histomorphological marker in assessing 69 cases tumour microcirculation in endometrial carcinoma and predict imaging markers of depth of myometrial invasion and assessment surgical methods.The permeability and blood flow in tumor was significantly lower,which may be related to the hypoxic environment. And the plasma and extravascular extracellular space volume in tumor are both lower, which is considered to be due to the increased tumor parenchymal cells.ATH model derived Veattained highest value,which is closest to the MVD, may provide an imaging marker for predicting depth of myometrial invasion and assessment surgical methods.
Introduction
To compare five pharmacokinetic models for the analysis of dynamic contrast enhanced (DCE) MRI and study the angiogenic profile based on histomorphological marker in assessing microcirculation and the depth of myometrial invasion in endometrial carcinoma.Methods
Preoperative pelvic DCE-MRI was performed in 69 patients(mean age, 52 years; age range, 24–78 years) in whom a uterine tumor was visible at MRI and histologically verified as endometrial carcinoma(Figure 1). Imaging was performed on a 1.5T MR(Achieva Nova Dual, Philips, Netherlands) using a sixteen-channel body coil.Pelvic DCE-MRI was acquired with T1 High Resolution Isotropic Volume Examination (THRIVE)sequence(TE/TR=2.1/4.4ms,FA=18˚,slice thickness=5mm, number of slices =1035) with a temporal resolution of 2.5 s and 5-min delay. Multiple precontrast images were also acquired with different FAs of 6, 12 and 18˚. ROI were drawn and the data was analyzed retrospectively using MItalytics (Fitpu Healthcare, Singapore), where Tofts, extended Tofts, adiabatic tissue homogeneity (ATH), conventional compartmental (CC) and distributed parameter (DP) models were utilized to calculate the tumor and normal myometrium. Immunohistochemical staining with CD105 allowed assessment of microvessel density (MVD) reflecting tumour angiogenesis. Transfer constant(Ktrans), efflux rate constant(Kep), Blood flow (F), permeability surface area product (PS), plasma space fractional volume (Vp), extravascular extracellular space fractional volume (Ve), and extraction fraction (E) were derived. For all the derived imaging parameters and MVD of the tumor and normal myometrium median values, with 95% CI of the median were calculated. And the parameters were compared using ROC analysis to differentiate tumor and normal myometrium.Results
An example of the parametric maps obtained with the proposed methods is shown in Figure 2. Permeability parameters Kep, E and PS in tumor were lower than normal myometrium(Figure 3). Areas under ROC curves(AUCs) (Figure 4)for PS were >0.7 in three models. And AUCs for E was >0.75 in DP model, >0.65 in ATH and CC models. Kep was >0.75 and >0.6 for Tofts and Extended Tofts models respectively. The difference in Ktrans between two tissues was not significant. F in tumor was slower, with all AUCs >0.7. Ve and Vp in tumor were significantly lower, Vp with AUC >0.75 for DP and CC models, and <0.6 for ATH and Extended Tofts models. AUCs for Ve attained the largest value with AUCs >0.8 for four models except CC model(AUC<0.65). ATH-derived Ve attained the largest AUC value of 0.8474.MVD in tumor was lower than the normal myometrium, with AUC value of 0.879.Discussion
In this study we have shown that preoperative functional DCE-MRI yield imaging parameters which could be markers of depth of myometrial invasion. This functional imaging techniques may thus represent valuable supplements to conventional pelvic MRI, enabling improved preoperative risk stratification facilitating better tailored surgical and adjuvant treatment in endometrial cancer patients. This is, to our knowledge, the first research comparing intra-tumour angiogenesis and myometrium microvessel function based on five different kinetic models of quantitative DCE-MRI in endometrial carcinoma patients. A fundamental difference between the various kinetic models stems from the assumption of homogeneous (well- mixed) or distributed compartments. The CC models assume homogeneous compartments, whereas the ATH and DP models assume a distributed vascular compartment. The main advantage of the Tofts model is its simplicity and perhaps the most widely used model for analysis of DCE MRI data. The extended Tofts model is a two-compartment model since it accounts for the vascular volume Vp. The AUC of Ve in all four models is bigger than 0.8, which indicate that its differentiation ability is relatively stable under the restrictions of different models. The ATH model has the highest AUC and is closest to the AUC value of MVD, which provide a clinical imaging marker for predicting surgical methods and prognosis. Interestingly, the permeability in tumor was significantly lower, which is somewhat puzzling, because the tumor vessels are generally considered more tortuous and leaky than normal vessels. This may suggest a very different cell growth mechanism in endometrial cancer, which may be related to the hypoxic environment. The hypoxic endothelial cells may cause the reduction in permeability.The low tumor blood flow (F) in our finding supporting the notion that reduced blood flow which is putatively linked to tissue hypoxia, is associated with tumor progression and aggressive disease.Also similar to a previous study(employing a different two-compartment model)found that lower F in endometrial cancer.The Ve and Vp in tumor was lower is considered to be due to the increased tumor parenchymal cells.conclusion
Endometrial carcinoma characterized by low permeability and low blood flow in comparison with most solid tumours. Of the models investigated, the ATH model was the best predictor of predict the depth of myometrial invasion in endometrial cancer patients.Acknowledgements
No acknowledgements.References
- Taxt T, Jirik R, Rygh CB, et al. Single-channel blind estimation of arterial input function and tissue impulse response in DCE-MRI. IEEE Trans Biomed Eng. 2012; 59(4): 1012–1021.
- Koh TS, Bisdas S, Koh DM, et al. Fundamentals of tracer kinetics for dynamic contrast-enhanced MRI. J Magn Reson Imaging 2011; 34(6):1262–1276.
- Casazza A, Di Conza G, Wenes M,et al.Tumor stroma: a complexity dictated by the hypoxic tumor microenvironment.Oncogene. 2014; 33(14):1743-1754.
- Haldorsen IS, Stefansson I, Gruner R, et al. Increased microvascular proliferation is negatively correlated to tumour blood flow and is associated with unfavourable outcome in endometrial carcinomas. Br JCancer. 2014; 110(1): 107–114.
Figures
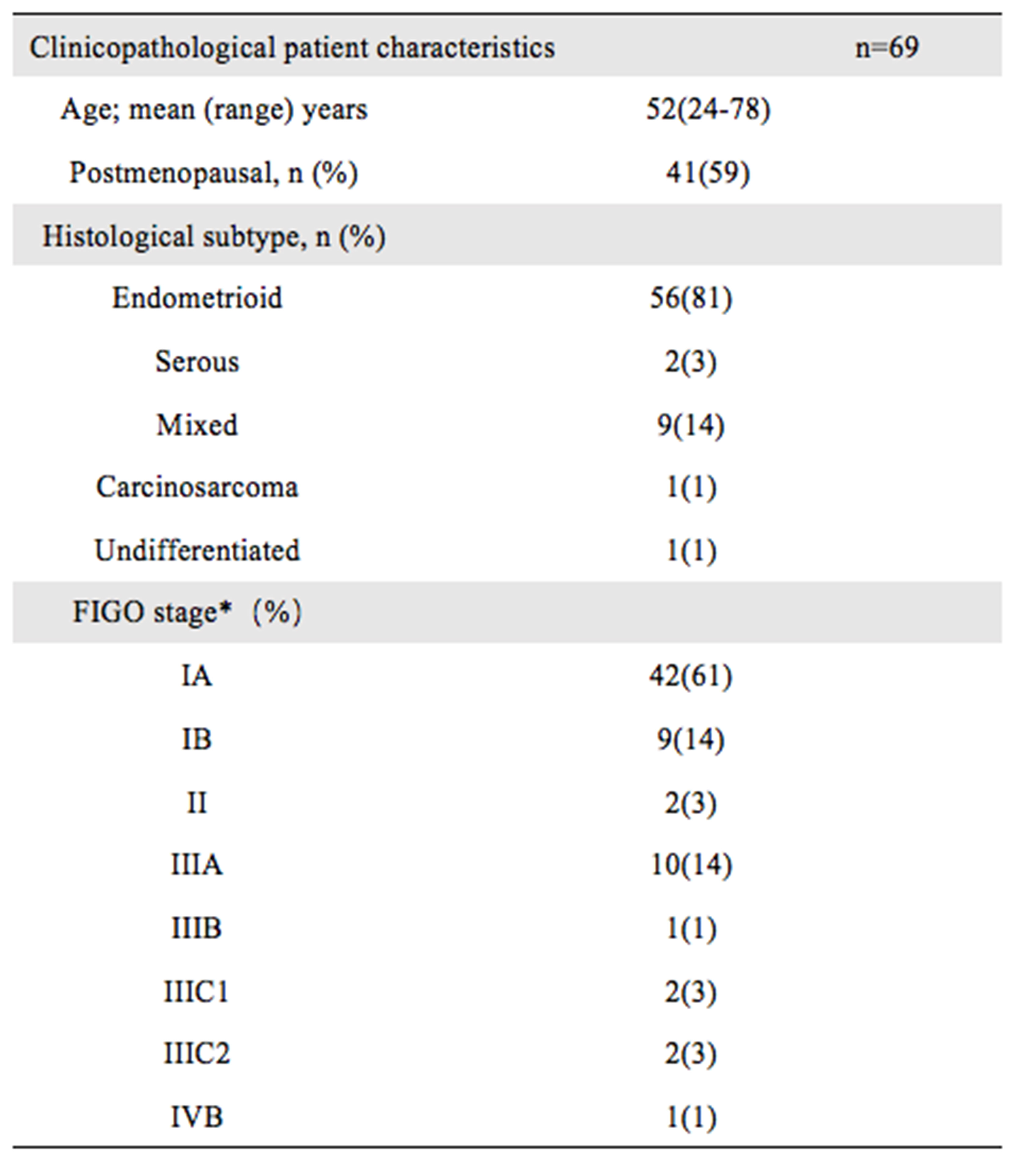
Clinicopathological patient characteristics.
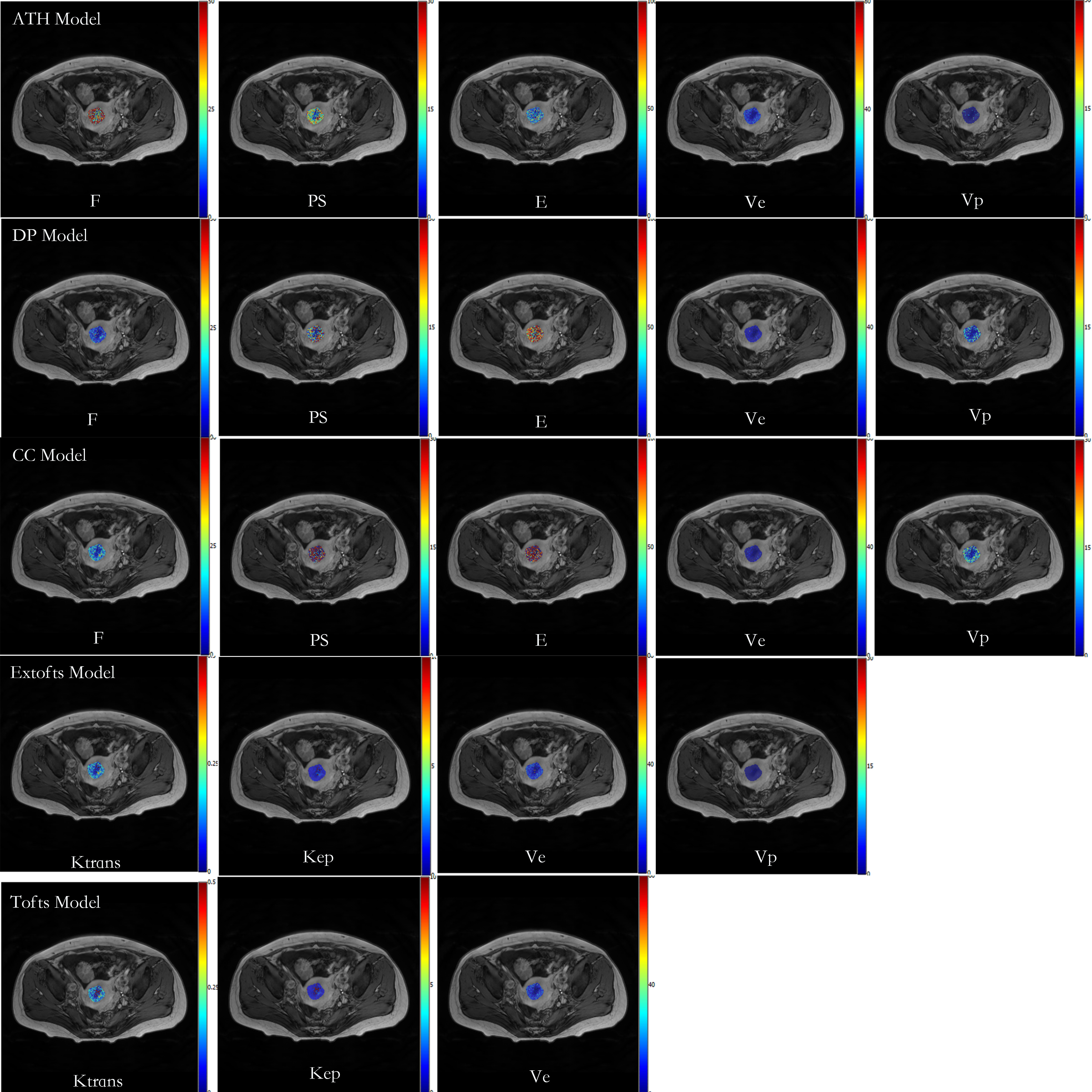
The parametric maps from DCE-MRI in a 39-year-old patient with endometrial carcinoma, FIGO stage IVB,grade 3.
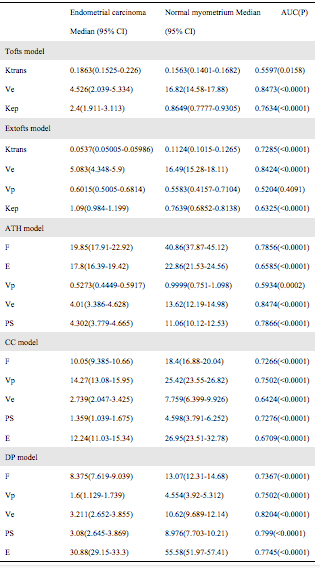
Quantitative DCE-MRI parameters and areas under ROC curves measured in ROIs within endometrial tumor tissue and in corresponding regions in normal myometrium (n=69).

Areas under ROC curves(AUCs) for parameters in 5 different models and MVD.