1824
Using kinetic parameters from DCE-MRI to differentiate endometrial adenocarcinoma from adenocarcinoma of cervixXiaoduo Yu1, Meng Lin1, Qi Zhang1, Lizhi Xie2, Yuqing Shang3, and Han Ou-Yang1
1Department of Diagnostic Radiology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2GE Healthcare, China, Beijing, China, 3Department of Chronic Disease Epidemiology, Yale School of Public Health, Yale University, New Haven, CT, United States
Synopsis
This study attempted to use parameters derived from DCE-MRI to quatitatively investigate the perfusion difference between adenocarcinoma of endometrium and cervix. It was concluded that values of kinetic parameters were lower in uterine endometrioid adenocarcinoma (EAC) and adenocarcinoma of cervix (AdC). When encountered uterine adenocarcinoma with uncertain biopsy pathology and a confusing morphology of MRI, DCE-MRI would be a reliable supplementary method to improve diagnostic confidence.
Purpose
To evaluate the values of kinetic parameters derived from dynamic contrast enhanced magnetic resonance imaging (DCE-MRI) in distinguishing uterine endometrioid adenocarcinoma (EAC) from adenocarcinoma of cervix (AdC) since they correspond to different diagnosis and prognosis.Introduction
Material
Sixty newly diagnosed patients with distinctive pathology underwent DCE-MRI before treatments. Two observers independently calculated the tumor diameters and the parameters of DCE-MRI (including quantitative parameters: Ktrans, Kep and Ve; semi-quantitative parameters: TTP (time to peak), Maxconc(initial area under the gadolinium curve), AUC (Initial area under the gadolinium curve) and Maxslop, using both population and individual based arterial input function (AIF). Inter-observer consistency was evaluated using intra-class correlation (ICC) and Bland-Altman plots. Comparisons between EAC and AdC were performed via Independent sample t-test or Mann–Whitney U test according to the normal distributions of data. Receiver operating characteristic (ROC) curve and area under curve (AUC) were used to analyze the diagnostic efficiency of significant parameters and those combinations.Results
Inter-observer reproducibility (ICC = 0.938-0.987) was excellent with relatively higher ICC and smaller SD on Bland-Altman plot, especially when calculated via population AIF(Fig.1). The tumor diameters were not correlated with tumor types. All the parameters, except Kep derived from population AIF and TTP derived from both sets of AIFs, were lower in EAC than in AdC. AUC is 0.895 on Ve and 0.888 on Maxconc when calculated with population AIF, and is 0.915 when calculated from the combination of Ve and Maxconc. The diagnostic efficiency to differentiate EAC with AdC achieved an accuracy level of 85.00% with Maxconc alone, and a specificity level of 90.91% with the combination of Ve and Maxconc(Fig.2, Fig.3).Discussion and Conclusion
The results of our study displayed significantly higher Ktrans, Maxconc, AUC and Maxslop in both sets of AIF in AdC when compared with those in EAC, indicating that AdC had higher perfusion than EAC, which were consistent with previous studies . The measurements by population AIF showed fairly good agreement with the smaller SD and 95% limits of agreement on Bland–Altman plots and the standard deviations of mean values of quantitative parameters were relatively larger when using individual AIF, therefore, population AIF was recommended with better repeatability. Our results suggested that the two adenocarcinomas may have similar TTP. The original small number of patients with inconclusive adenocarcinoma by cervical biopsy, posed challenges to collect patients, especially with unified sequence. Therefore, we have to add some patients with distinctive EACs confirmed by endometrial curettage, which maybe lead to insignificance in morphological evaluation, and needed more case in further study. In conclusion, DCE-MRI could be used as a reliable supplementary MRI method for quantitatively evaluating the perfusion difference between the EAC and AdC, and to assist the diagnosis determination of uterine adenocarcinoma with uncertain biopsy pathology.Acknowledgements
No acknowledgement found.References
[1] Pecorelli S, Pasinetti B, Angioli R, et al. Systemic therapy for gynecological neoplasms: ovary, cervix, and endometrium. Cancer Chemother Biol Response Modif.2005, 22:515-544.[2] Khoury T, Tan D, Wang J, et al. Inclusion of MUC1 (Ma695) in a panel of immunohistochemical markers is useful for distinguishing between endocervical and endometrial mucinous adenocarcinoma. BMC Clin Pathol.2006,6:1.
[3] He H, Bhosale P, Wei W, et al. MRI is highly specific in determining primary cervical versus endometrial cancer when biopsy results are inconclusive. Clin Radiol.2013, 68(11):1107-1113.
[4] Ramirez PT, Frumovitz M, Milam MR, et al. Limited utility of magnetic resonance imaging in determining the primary site of disease in patients with inconclusive endometrial biopsy. Int J Gynecol Cancer.2010, 20(8):1344-1349.
[5] Bourgioti C, Chatoupis K, Panourgias E, et al. Endometrial vs. cervical cancer: development and pilot testing of a magnetic resonance imaging (MRI) scoring system for predicting tumor origin of uterine carcinomas of indeterminate histology. Abdom Imaging.2015, 40(7):2529-2540.
Figures
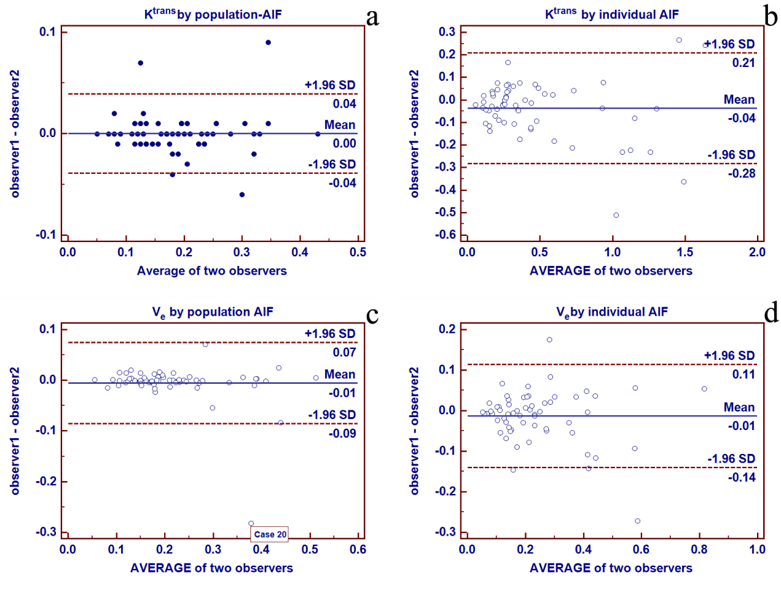
Fig.1
Bland–Altman plots together with 95% CI of DCE-MRI parameters inter-observers
Bland-Altman
plots of Ktrans measured from two observers using population AIF (a),
Ktrans of two observers using individual AIF (b), Ve
of two observers using population AIF (c), Ve of two
observers using individual AIF (d). Solid line and adjacent number indicate the
mean difference, anddash line and
adjacent number indicate the limits of
agreement. The measurements of quantitative parameters using population AIF (a,
c) showed smaller mean difference than those using individual AIF (b,d).
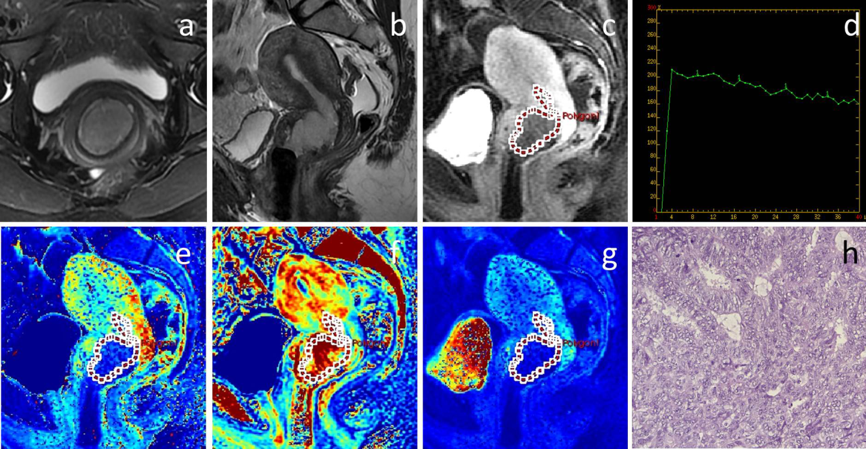
Fig.2
F40, (a) axial T2-weighted with fat saturation and (b) sagittal T2-weighted
imaging demonstrated that the tumor bulk is mainly located
in the cervix and invaded into the
uterus corpus along the endometrium cavity with heterogeneously high intensity
signal. (c) DCE-MRI equilibrium phase presented homogeneous enhancement and
lower intensity signal than myometrium. (d) TIC processed by AW Workstation , showed the enhanced
peak in the arterial phase (the fourth phase)
with TTP of 24s. (e) Ve map (f) Kep map and (g) Maxconc
map derived from DCE-MRI were0.15, 0.96min-1 and 0.25mmolmin, respectively. Surgical specimen indicated that tumor
originated from lower uterine segment. Histology (h) revealed moderately
differentiated endometrioid adenocarcinoma (hematoxylin–eosin stain;
original magnification, ×100), which was composed of glands similar to normal
endometrium.
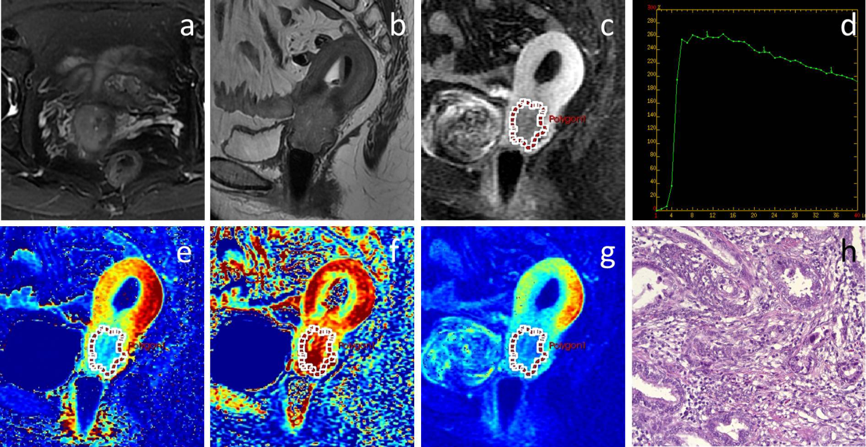
Fig.3
F45, (a) axial T2-weighted with fat saturation and (b) sagittal T2-weighted
imaging demonstrated that the tumor bulk is mainly located in the cervix and
invaded into the uterus corpus with heterogeneously high intensity signal. (c)
DCE-MRI equilibrium phase presented homogeneous enhancement and lower signal
intensity than myometirum. (d) TIC showed the enhanced peak in the arterial
phase (the fourth phase) with TTP of 36s. (e) Ve map (f) Kep map (g) Maxconc map derived from DCE-MRI were 0.34,
0.95min-1 and 0.51mmolmin, respectively. The patient conducted
surgery after neoadjuvant chemotherapy, and histological specimen (h) revealed
poorly and moderately differentiated cervical adenocarcinoma (hematoxylin–eosin
stain; original magnification, ×100), which was composed of multiple neoplastic
gland that is rich of mucin.