1822
Preoperative prediction of lymph node metastasis in rectal cancer by multiregional radiomics features from multiparametric MRI1Department of Radiology, The First Hospital of Jilin University, changchun 130021, China, 2Philips Healthcare, Beijing, China
Synopsis
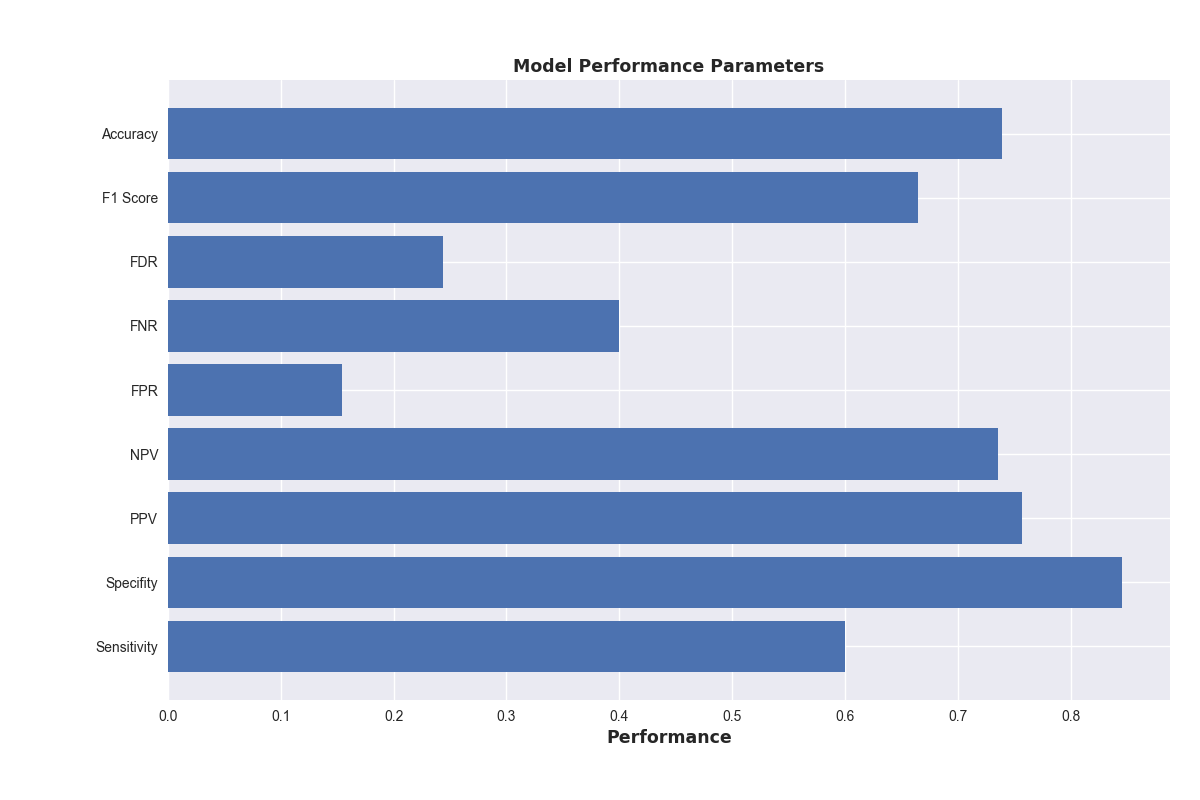
Preoperative accurate assessment of lymph node (LN) status in rectal cancer is essential for precise individualized decision-making. Nevertheless, preoperative LN staging in rectal cancer remains a challenge for the radiologist. Therefore, we develop and validate a radiomics prediction model based on MRI for the preoperative individualized prediction of LN metastasis. The Ridge Classifier is found to give the best prediction accuracy score(73.9%).The mean specificity, sensitivity and F1 score are 84.6%, 60% and 66.4 % , respectively. So, radiomics features from MRI of rectal cancer is a useful tool for predicting LN metastasis preoperatively and has marked discrimination accuracy.
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed malignancy and the fourth leading cause of cancer death in the world.1,2 Preoperative accurate assessment of lymph node (LN) status in rectal cancer via imaging is essential for precise individualized decision-making. Local excisional procedures are appropriate as a single modality for early cancers (cT1N0 without adverse features). 3-7 Nevertheless, preoperative LN staging in rectal cancer remains a challenge for the radiologist.5 Pelvic MRI is considered to be the most accurate method to assess locoregional clinical staging, and should be applied to define the extent of surgery. 3A meta-analysis noted that neither currently used imaging modalities can reliably evaluate LN metastasis.3,5,8 All modalities rely heavily on the criterion of size, and size on its own is insufficient to reliably distinguish between malignant and benign LN in rectal cancer.3,5,6,9 Radiomics, the high-throughput mining of quantitative image features from standard-of-care medical imaging that enables data to be extracted and applied within clinical-decision support systems to improve diagnostic, prognostic, and predictive accuracy, is gaining importance in cancer research.10-13 It is of interest that whether there exists an association between the LN status and radiomics features of MR images, which to the best of our knowledge has not been studied. Therefore, the aim of this study was to develop and validate a radiomics prediction model based on MRI for the preoperative individualized prediction of LN metastasis, accordingly the clinicians can make a personalized treatment plan.Methods
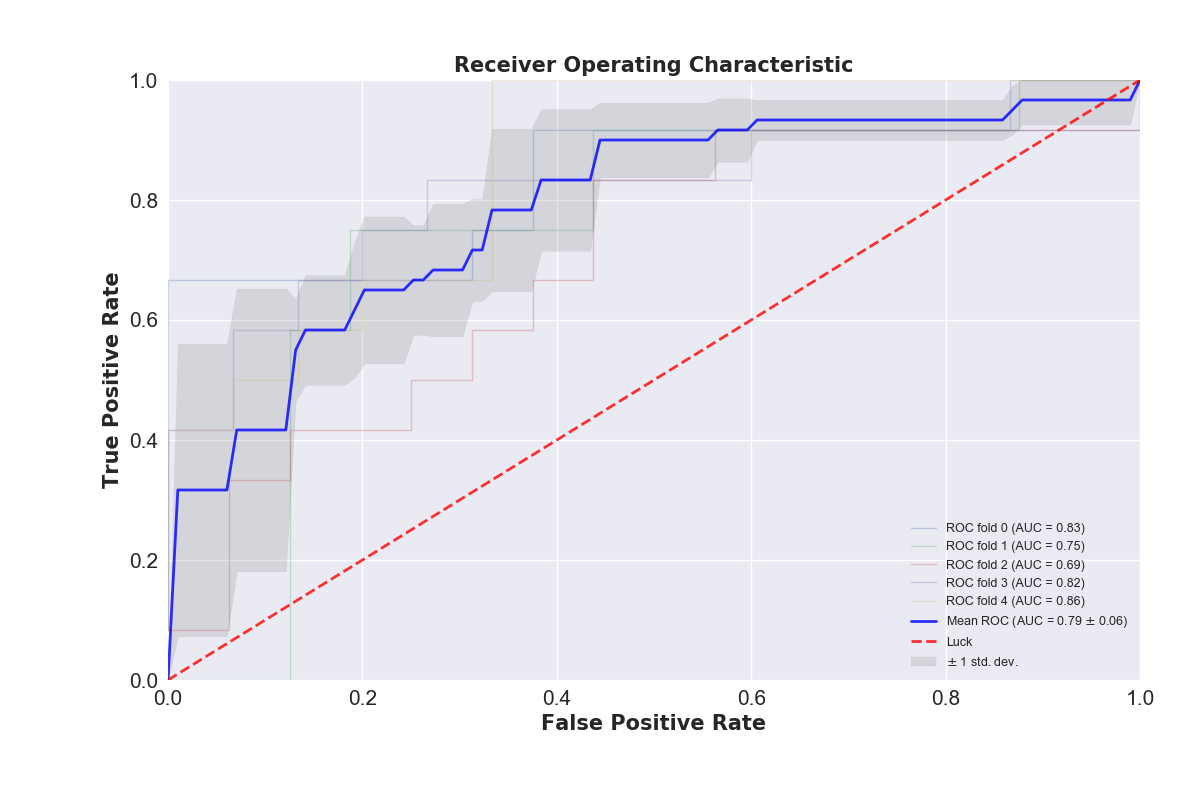
A total of 138 rectal cancer patients who underwent radical surgical resection with pathological results between Jan. 2016 and Jan. 2018 were included in this study. All the patients underwent rectal MRI (T2-weighted and diffusion-weighted imaging) scan before the surgery. Multivariate models were trained on the training cohort and their performance was evaluated on the 5-fold cross-validation cohort using the area under ROC curve (AUC), accuracy, specificity and sensitivity. The regions of interest (ROIs) is defined as follows: a. the volume of the whole primary tumor, which were created manually based on T2WI and DWI; b. the volume of mesorectal region on T2WI. We use three different series of region of interest (ROI) in Radiomics feature calculation, including lesions of tumor and mesorectum on T2 image and lesions of tumor on DWI image drawn by one radiologist using IntelliSpace Discovery (Philips, Best, the Netherlands) and analyzed by Philips Radiomics Tool (Philips Healthcare, China, the core feature calculation is based on pyRadiomics). For each ROI, a total of 1227 three-dimensional (3D) based radiomic features were extracted. These radiomic features quantified tumor characteristics using tumor size and shape, intensity statistics, and texture. For each patient, we integrated all of the 3681 Radiomics features from three ROIs together. In the following feature dimension reduction analysis, we used Pearson correlation, hierarchical cluster analysis and principal component analysis (PCA) to select the key features. In modeling stage, we investigated 19 classification methods (including Passive Aggressive Classifier, Perceptron, Ridge Classifier, SGD Classifier, Logistic Regression, AdaBoost Classifier, Bagging Classifier, Extra Trees Classifier, Gradient Boosting Classifier, Random Forest Classifier, K Neighbors Classifier, Support Vector Classifier, Decision Tree Classifier, Linear Discriminant Analysis, Quadratic Discriminant Analysis, MLP Classifier, XGB Classifier, Extra Tree Classifier, Gaussian Process Classifier) for training and prediction. These models were trained on the training cohort and their performance was evaluated on the cross-validation cohort using the area under ROC curve (AUC).Result and discussion
Among the 19 machine learning models, the Ridge Classifier is found to give the best prediction accuracy score, the mean value of which is 73.9%. Meanwhile, the mean specificity, sensitivity and F1 score are 84.6%, 60% and 66.4 % , respectively (Figure 3). We developed and validated a radiomics model for the preoperative individualized prediction of lymph node metastasis in patients with rectal cancer with high accuracy, specificity and sensitivity.Conclusion
Multiparametric radiomics features from multiparametric MRI of rectal cancer is a useful tool for predicting lymph node metastasis preoperatively and has marked discrimination accuracy.Acknowledgements
No acknowledgement found.References
1. Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut. 2017;66(4):683-91.
2. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International journal of cancer. 2015;136(5):E359-86.
3. Glynne-Jones R, Wyrwicz L, Tiret E, et al. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of oncology : official journal of the European Society for Medical Oncology. 2017;28(suppl_4):iv22-iv40.
4. Chen LD, Liang JY, Wu H, et al. Multiparametric radiomics improve prediction of lymph node metastasis of rectal cancer compared with conventional radiomics. Life sciences. 2018;208:55-63.
5. Lahaye MJ, Beets GL, Engelen SM et al (2009) Locally advanced rectal cancer: MR imaging for restaging after neoadjuvant radiation therapy with concomitant chemotherapy. Part II. What are the criteria to predict involved lymph nodes? Radiology 252:81–91.
6. Nougaret S, Reinhold C, Mikhael HW, Rouanet P, BibeauF, Brown G. The use of MR imaging in treatmentplanning for patients with rectal carcinoma: have youchecked the “DISTANCE”? Radiology 2013; 268:330–44.
7. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) in Colon Cancer (Version 1.2017). Available at: http://wwwnccnorg/professionals/physician_gls/f_ guidelinesasp. 2017.
8. X.T. Li, Y.S. Sun, L. Tang, K. Cao, X.Y. Zhang, Evaluating local lymph node metastasis with magnetic resonance imaging, endoluminal ultrasound and computed tomography in rectal cancer: a meta-analysis, Color. Dis. 17 (2015)O129–O135.
9. Horvat N, Veeraraghavan H, Khan M, et al. MR Imaging of Rectal Cancer: Radiomics Analysis to Assess Treatment Response after Neoadjuvant Therapy. Radiology. 2018;287(3):833-43.
10. Gillies RJ, Kinahan PE, Hricak H: Radiomics: Images are more than pictures, they are data.Radiology 278:563-577, 2016.
11. Lambin P, Leijenaar RTH, Deist TM, et al. Radiomics: the bridge between medical imaging and personalized medicine. Nature reviews Clinical oncology. 2017;14(12):749-62.
12. Horvat N, Veeraraghavan H, Khan M, et al. MR Imaging of Rectal Cancer: Radiomics Analysis to Assess Treatment Response after Neoadjuvant Therapy. Radiology. 2018;287(3):833-43.
13. Limkin EJ, Sun R, Dercle L, et al. Promises and challenges for the implementation of computational medical imaging (radiomics) in oncology. Annals of oncology : official journal of the European Society for Medical Oncology. 2017;28(6):1191-206.
Figures
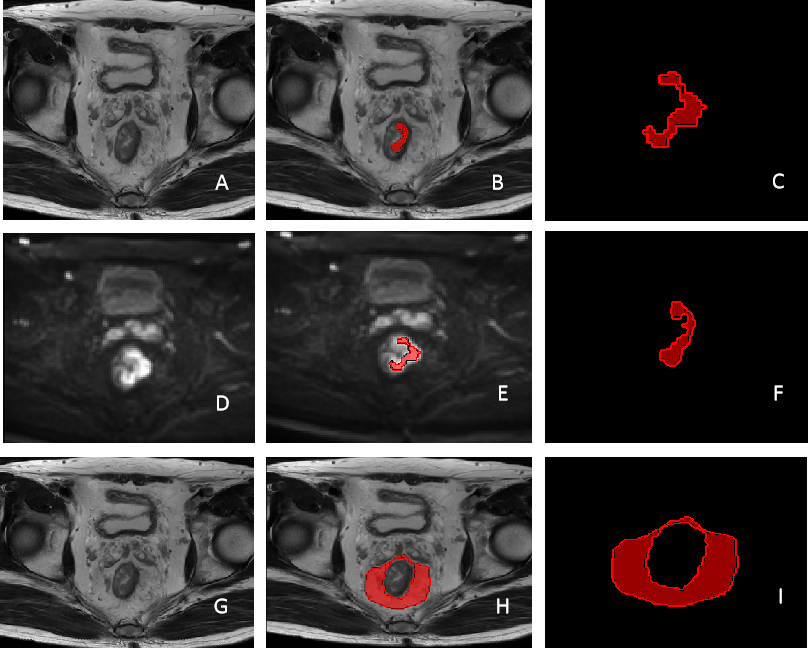
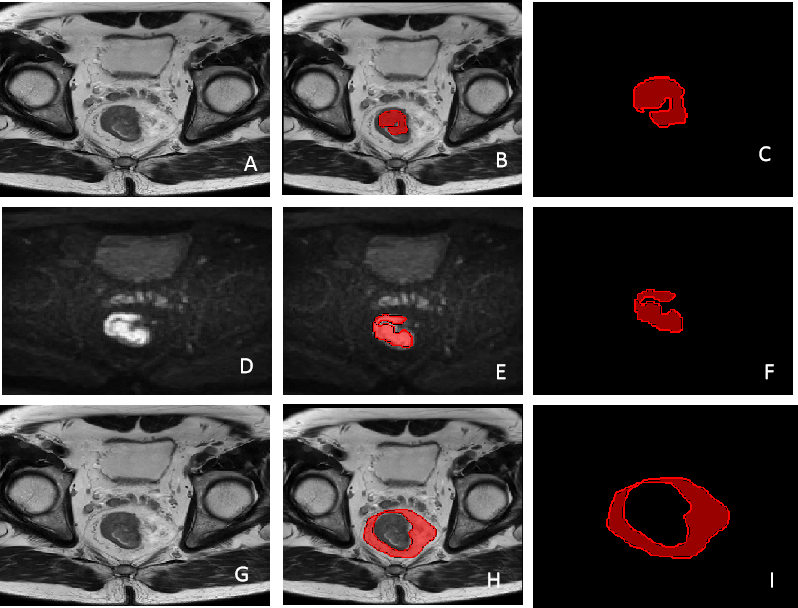
Figure1 The segmentation result of tumor and mesorectum on T2WI and DWI in a LN-positive patient. Images in a 62- year-old male, LN-positive rectal cancer.(A), (B), (C): the ROIs of primary tumor on T2WI; (D), (E), (F): the ROIs of primary tumor on DWI; (G), (H), (I): The ROIs of mesorectum on T2WI.