1814
A radiomics approach to assess tumor-stromal ratio and predict treatment response to neoadjuvant chemoradiotherapy in rectal cancer: a preliminary study1Department of Radiology, Fudan University Shanghai Cancer Center, Shanghai, China, 2Department of Pathology, Fudan University Shanghai Cancer Center, Shanghai, China
Synopsis
This study concentrated on the correlation between radiomics parameters and the tumor-stromal ratio. We identified several radiomics parameters that may reflect the content of tumor-stroma. After constructed a radiomics signature based on the tumor-stromal ratio and furtherly applied the signature into the LARC patients with neoadjuvant chemoradiotherapy, we found that the TSR-conducted radiomics signature was significantly correlated with pCR and non-pCR. The radiomics signature may serve as a non-invasive imaging biomarker for pretreatment prediction of treatment response.
Abstract
Background:Tumor stroma, as a component of the microenvironment of cancer, has previously been reported to affect tumor cell signalling, survival, proliferation and drug sensitivity$$[1]$$. Many investigators have researched that the tumor stromal ratio(TSR) is an independent, poor prognostic factor in rectal cancer$$[2-4]$$. Innovative and noninvasive predictors of the TSR are needed to guide clinical treatment and improve patients outcomes. The purpose of our study is to research whether MRI radiomics parameters vary according to tumor-stroma ratio in rectal cancer patients, and whether the TSR-conducted radiomics signature can predict treatment response to neoadjuvant chemoradiotherapy (CRT).
Methods:Institutional review board approval was obtained, and patient consent was waived. In this retrospective study, we enrolled two cohorts of rectal cancer patients with pelvic magnetic resonance (MR) imaging and diffusion-weighted (DW) imaging before any treatment and surgery in our institution database. Firstly, to develop the radiomic signature of TSR, we used a total of 159 resected rectal cancer patients between June 1, 2016 to May 30, 2018. TSR was determined on hematoxylin and eosin stained histological sections. Two pathologists evaluated the TSR and divided the patients into stroma-rich group (TSR≥50%) and stroma-poor group(TSR<50%). A total of 129 radiomics features were assessed from contrast-enhanced T1, T2 and diffusion-weighted images by the LIFEx. The univariate logistic regression analyses were performed to identify the independent features correlated with TSR, and the significant features were introduced into the multivariate logistic regression model to construct the radiomics signature of TSR.
Secondly, to research the relationship between the TSR-conducted radiomics signature and treatment response after CRT, we enrolled a total of 180 locally advanced rectal cancer (LARC) patients between January 1, 2015 to April 30, 2018. All patients received preoperative adjuvant chemoradiotherapy followed by TME. Pathological response to CRT was assessed using the Tumor Regression Grade (TRG) by two experienced pathologist. 129 radiomics parameters were extracted and the radiomics signature was calculated with the formula derived from the multivariate regression model. Univariate logistic regression was applied to identify the relationship between treatment response and the TSR-conducted radiomics signature.
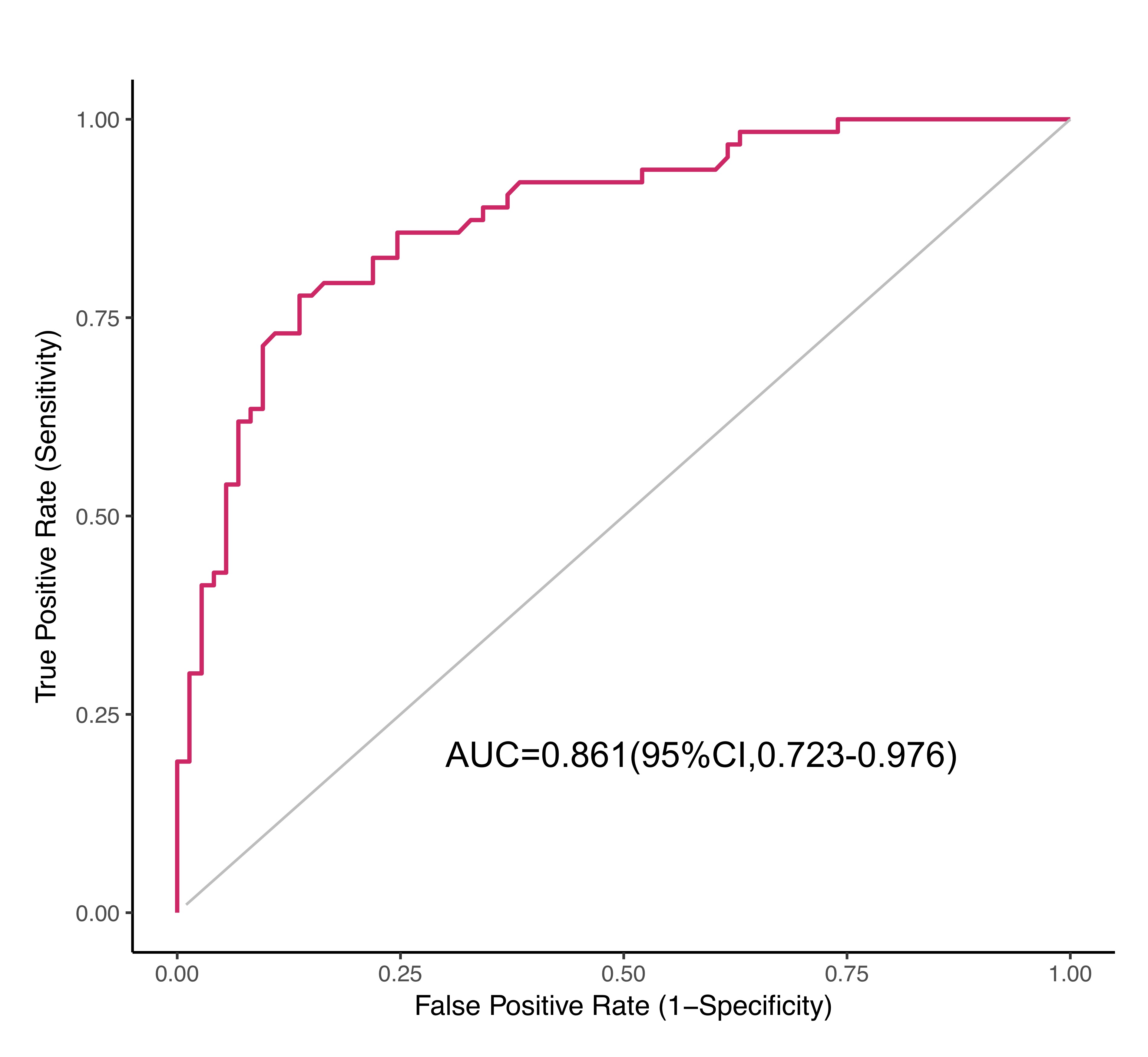
Results:Univariate logistic regression selected 7 radiomics parameters correlated with TSR, the LRE (p=0.016), Homogeneity (p=0.035) and Energy (p=0.025) extracted from contrast-enhanced T1WI, the Contrast (p=0.029) and Entropy (p=0.033) extracted from T2WI, the RLUN(p=0.025) and Dissimilarity(p=0.029) extracted from DWI. After multivariate regression, the radiomics signature was constructed with RLUN (OR=1.031, 95%CI:1.001-1.062, p=0.043) and LRE (OR=0.945, 95%CI:0.895-0.997, p=0.039), and showed good discrimination with an area under the receiver operating characteristic curve of 0.861 (95% CI, 0.723–0.976). After calculating the radiomics signature for LARC patients, detectability was not significantly different between responders(TRG 0-1) and non-responders(TRG 2-3)(p=0.097) but significantly correlated with pCR(TRG 0) and non-pCR(TRG 1-3) (p=0.032). The signature also achieved good discrimination with AUC of 0.744(95% CI, 0.546–0.943).
Conclusions:MRI radiomics parameters showed significant differences according to the tumor- stroma ratio. The TSR-conducted radiomics signature can also predict treatment response to neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Thenon-invasiveimaging predictormay provide a promising way to guide clinical treatment when validated by further prospective randomised trials.
Acknowledgements
No acknowledgement found.References
1. McMillin DW, Negri JM, Mitsiades CS (2013) The role of tumour-stromal interactions in modifying drug response: challenges and opportunities. Nat Rev Drug Discov 12:217-2282
2. Eriksen AC, Sorensen FB, Lindebjerg J et al (2018) The prognostic value of tumour stroma ratio and tumour budding in stage II colon cancer. A nationwide population-based study. Int J Colorectal Dis 33:1115-11243
3. Park JH, Richards CH, McMillan DC, Horgan PG, Roxburgh CS (2014) The relationship between tumour stroma percentage, the tumour microenvironment and survival in patients with primary operable colorectal cancer. Ann Oncol 25:644-6514
4.Huijbers A, Tollenaar RA, v Pelt GW et al (2013) The proportion of tumor-stroma as a strong prognosticator for stage II and III colon cancer patients: validation in the VICTOR trial. Ann Oncol 24:179-185
Figures