1801
Liver mDixon at 7T1University of Nottingham, Nottingham, United Kingdom, 2Sir Peter Mansfield Imaging Centre, School of Physics and Astronomy, University of Nottingham, Nottingham, United Kingdom
Synopsis
mDixon imaging can provide robust anatomical images at 7T. These images have also been used to provide preliminary initial measurements of fat fraction in the liver at 7T.
Introduction
Parallel transmit technology (pTx) and novel transmit coil design has made abdominal imaging at 7T possible [1]. 7T has the potential to produce high quality anatomical images and fat quantification to provide increased sensitivity to detect changes related to conditions such as non-alcoholic fatty liver disease (NAFLD). However, the increase in SNR available at higher magnetic fields comes at a cost. The shorter RF wavelengths (~12cm) lead to destructive interference patterns that present significant challenges for achieving homogenous B1+ excitation and uniform contrast and signal intensity. The mDixon algorithm normalizes the images which overcomes some of the variations in signal intensity.Aim
To explore the potential of mDixon images to provide workhorse
anatomical scans with reduced signal drop out at 7T and to obtain preliminary
fat quantification maps of the liver.
Methods
Abdominal imaging was carried out on healthy
volunteers using a Phillips 7T Achieva 8-channel multi-transmit system with an
8 channel transmit, 32 channel receive fractionated dipole body array [2] (MR
Coils, Zaltbommel, Netherlands). B0 shimming was implemented using the Philips
volume shimtool over a region encompassing the liver. RF shimming was also
performed using a phase nulling method to maximise the B1+ in regions of
interest also encompassing the liver.
Preliminary fat quantification was performed on two healthy volunteers. Following the recommendations of Reeder et al 2005 [1], 3D multi gradient echo images were acquired at 6 echo times (TE1=1.4ms, rTE=1.32ms), a field of view (FOV) of 400 x 400 mm2 with 4 slices of resolution 2 mm x 2 mm x 5 mm (with in-plane reconstruction 0.93 x 0.93 mm2). Images were acquired during a single breath hold (maximum 30 s). The magnitude signal was fitted to a 6 peak model using non-linear least squares fit in Matlab assuming a single R2* for fat and water.
S = ( W + F ΣCi exp(jωit)) exp( j(Ψt+φ) - R2*t)
![]()
S is complex signal for n components varying with time t where Si= component signal, ωi= component resonant frequency, Ψ= local field offset, φ= constant phase offset, R2*= component relaxation, W = water signal, F = fat signal with m fat peaks ci= proportional amplitude constant at ωi resonant frequency where Σci=1.
The average fat fraction was measured in an ROI where the signal in the base
multiecho images was high.
Results
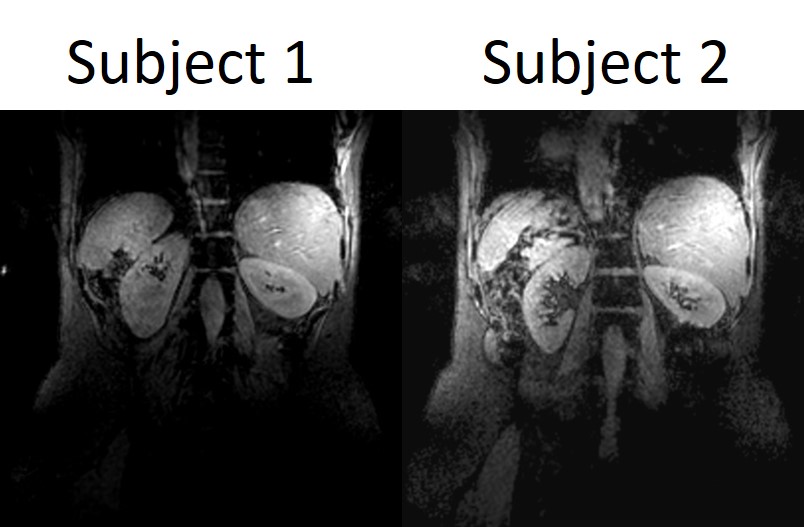
Figure 1 shows in vivo coronal water only calculated images
covering the kidneys and part of the liver. Figure 2 shows the fat, water,
in-phase and opposed-phase images generated over the liver in the transverse
plane. Figure 3 show the liver and part of the bowel surrounded by fat in the
transverse plane. Figure 4 shows the magnitude signal from the first echo of
the fat quantification acquisition along with the fat fraction maps. The fat
fraction calculated for subject 1 was 4.0%, and the fat fraction calculated for
subject 2 was 1.7%.
Discussion
High
quality, normalized mDIXON images were obtained from several subjects and highlight
the potential for mDIXON to be used as a rapid workhorse anatomical reference
scan at 7T. Promising results were seen across several areas in the body
including the kidneys, liver and bowel.
Accurate fat quantification proves a challenge at 7T.
The magnitude fitting used here has the advantage over fitting complex data in
that it is less affected by shimming errors. These are likely to be more of a
problem at 7T, given that the gradients available do not allow us to shorten
the echo time as the frequency shift between water and fat increases. However magnitude
imaging miscalculates fat fractions above 50%, so that any fraction above this
is misreported as a high water voxel. Despite this the preliminary maps are promising
and show that at 7T in vivo fat quantification is feasible.
Conclusions
Multiecho
acquisition with MDIXON reconstruction can provide a robust set of work horse
images for body rapid imaging at 7T. It has also been used for preliminary
measurement of fat fraction at 7T.
Acknowledgements
This work is funded by the Medical Research Council.References
- 1. Vaughan et al, Whole-Body Imaging at 7T: Preliminary Results, MRM. 2009;61:244-248
- 1. Raaijmakers et al, The Fractionated Dipole Antenna: A New Antenna for Body Imaging at 7 Tesla, MRM. 2016;75:1366-1374
- Reeder, S.B., et al., Iterative decomposition of water and fat with echo asymmetry and least-squares estimation (IDEAL): Application with fast spin-echo imaging. Magnetic Resonance in Medicine, 2005. 54(3): p. 636-644.
Figures