1792
Motion-Robust and Blood-Suppressed M1-Optimized Diffusion MR Imaging of the Liver1Medical Physics, University of Wisconsin Madison, madison, WI, United States, 2Radiology, University of Wisconsin Madison, madison, WI, United States, 3Laboratorio de Procesado de Imagen, Universidad de Valladolid, Valladolid, Spain
Synopsis
Liver DWI is complicated by multiple challenges, including the relatively short T2 of liver tissue and the motion sensitivity of diffusion encoding sequences. In this study, a novel approach for the design of diffusion weighting waveforms, termed M1-Optimized Diffusion Imaging (MODI), is proposed for motion-robust, blood-suppressed liver DWI. MODI includes an echo-time optimized motion-robust diffusion weighting gradient waveform design, with a moderate non-zero first-moment (M1≠0) value to enable blood signal suppression. This work describes the proposed MODI method, and evaluates its effectiveness in healthy volunteers as well as in patients.
Introduction
Liver DWI has been shown to enable the detection, characterization and treatment monitoring of focal liver lesions, as well as the assessment of diffuse liver disease (eg: fibrosis and cirrhosis)1,2. However, liver DWI is challenging because of the relatively short T2 of liver tissue and the motion sensitivity of diffusion encoding sequences3,4. Motion-induced phase dispersion results in signal voids in the DW images and bias in quantitative apparent diffusion coefficient (ADC) measurements. Recently, advanced motion-robust DW gradient waveform design techniques5-7 enabled first motion moment-nulled (M1-nulled) and/or second motion moment nulled (M2-nulled) DWI with optimized (i.e., minimum) echo time (TE). However, these motion moment-nulled gradient waveforms also compensate the signal from moving blood, which is nulled in standard liver DWI. Importantly, non-suppressed blood signal can mimic focal liver lesions and may confound the assessment and detection of true focal lesions in DWI, as well as introduce bias and variability in quantitative diffusion measures. Consequently, the lack of blood suppression in motion moment-nulled DWI techniques may hinder their clinical applicability for liver DWI.Theory
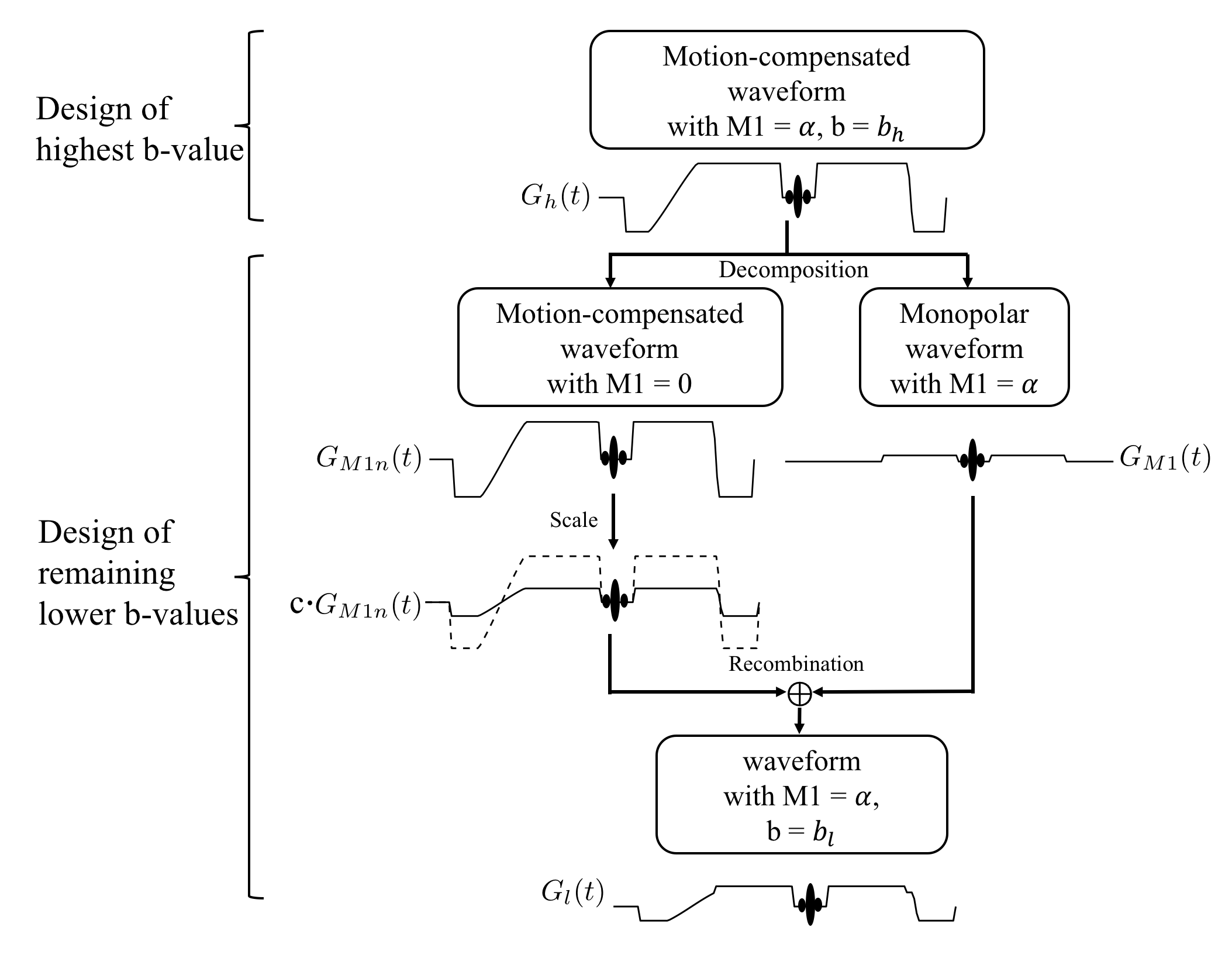
A novel approach for the design of diffusion weighting waveforms, termed M1-Optimized Diffusion Imaging (MODI), is proposed. MODI includes an echo-time optimized motion-robust diffusion weighting gradient waveform design, with a moderate non-zero first-moment (M1≠0) value to enable blood signal suppression. First, a desired high b-value b$$${_h}$$$ waveform is achieved by modifying the gradient optimization formulation proposed by Peña-Nogales Ó., et al6 to include a pre-specified, non-zero M1 = $$${\alpha}$$$ s/mm. The remaining lower b-values are designed following Fig.1. Because of the linearity of M1 as a function of the gradient waveform, $$${G_h(t)}$$$ can be decomposed into two waveforms $$${G_{M1n}(t)}$$$ and $$${G_{M1}(t)}$$$. $$${G_{M1n}(t)}$$$ can be scaled to the desired amplitude $$${c {\cdot} G_{M1n}(t)}$$$ and then recombined with $$${G_{M1}(t)}$$$ to achieve the desired low b-value b$$${_l}$$$.Methods
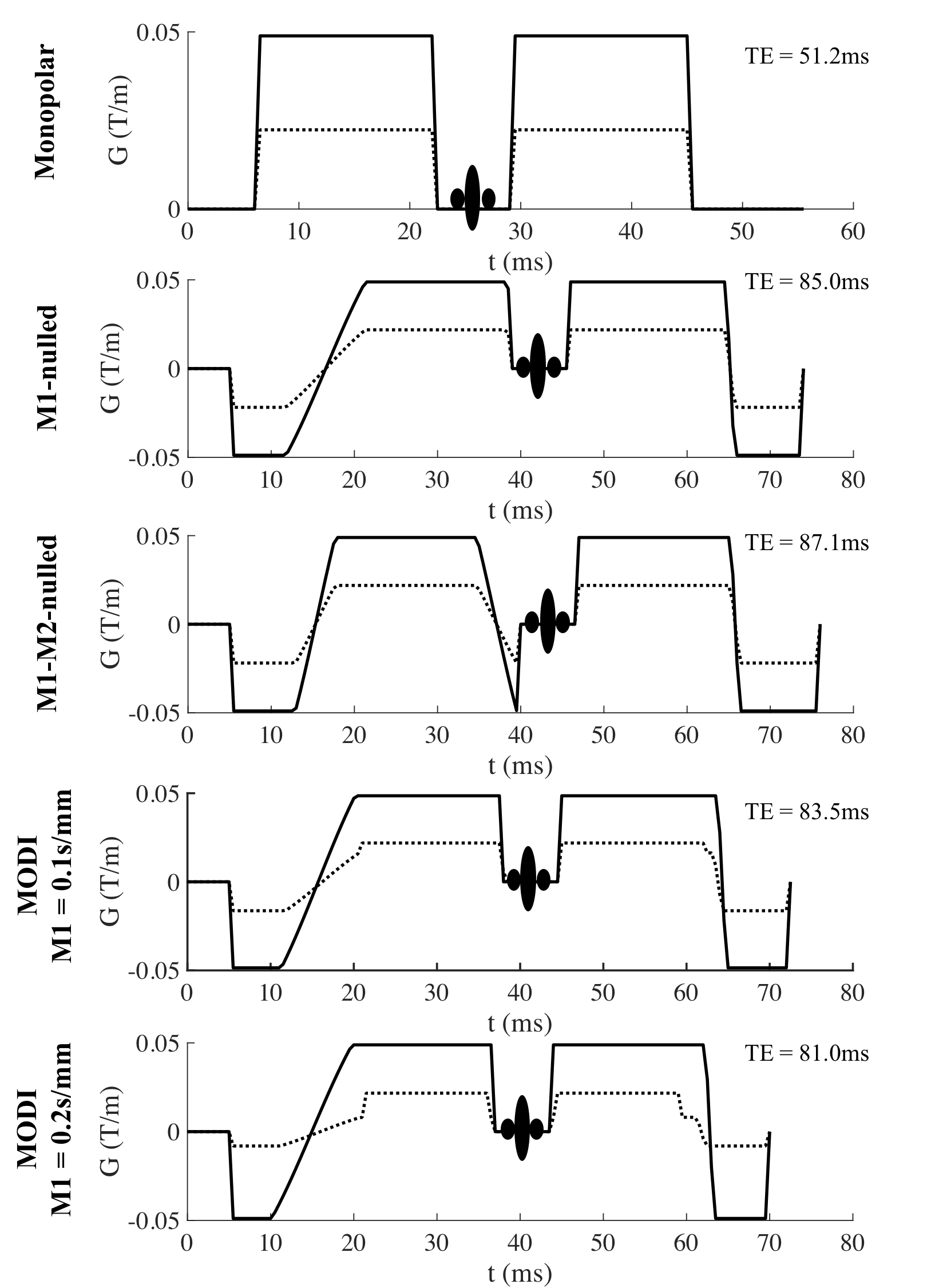
Waveform design: Four optimized waveforms were constructed and compared to the conventional monopolar diffusion encoding waveform (Fig.2). The four waveforms included two motion-compensated waveforms6 with M1-nulling and M1-M2-nulling, respectively, as well as two MODI waveforms. MODI waveforms were constructed with M1 = 0.1s/mm and M1 = 0.2s/mm, corresponding to a typical M1 value of the conventional Stejskal-Tanner monopolar diffusion gradients with b-values between b = 50 s/mm$$${^2}$$$ and b = 100 s/mm$$${^2}$$$, respectively. All the constructed waveforms were optimized with concomitant gradient nulling to avoid ADC bias6.
Healthy volunteer experiments: Eight healthy volunteers provided written consent for this IRB approved study. Volunteers were scanned on a 3T scanner (GE MR750 Waukesha, WI) with a 32-channel torso coil (Neocoil, Pewaukee, WI). The five waveforms shown in Fig.2 were acquired with b(#average)=[100(4), 500(8)]s/mm2, diffusion direction = three orthogonal directions, FOV=32cm$$${\times}$$$32cm, in-plane resolution = 2.5mm$$${\times}$$$2.5mm, slice thickness=6mm, bandwidth=$$${\pm}$$$250kHz, partial Fourier acquisition and respiratory triggering. For each acquisition, ADC maps were calculated and co-localized ROIs were drawn in each of the nine Couinaud liver segments.
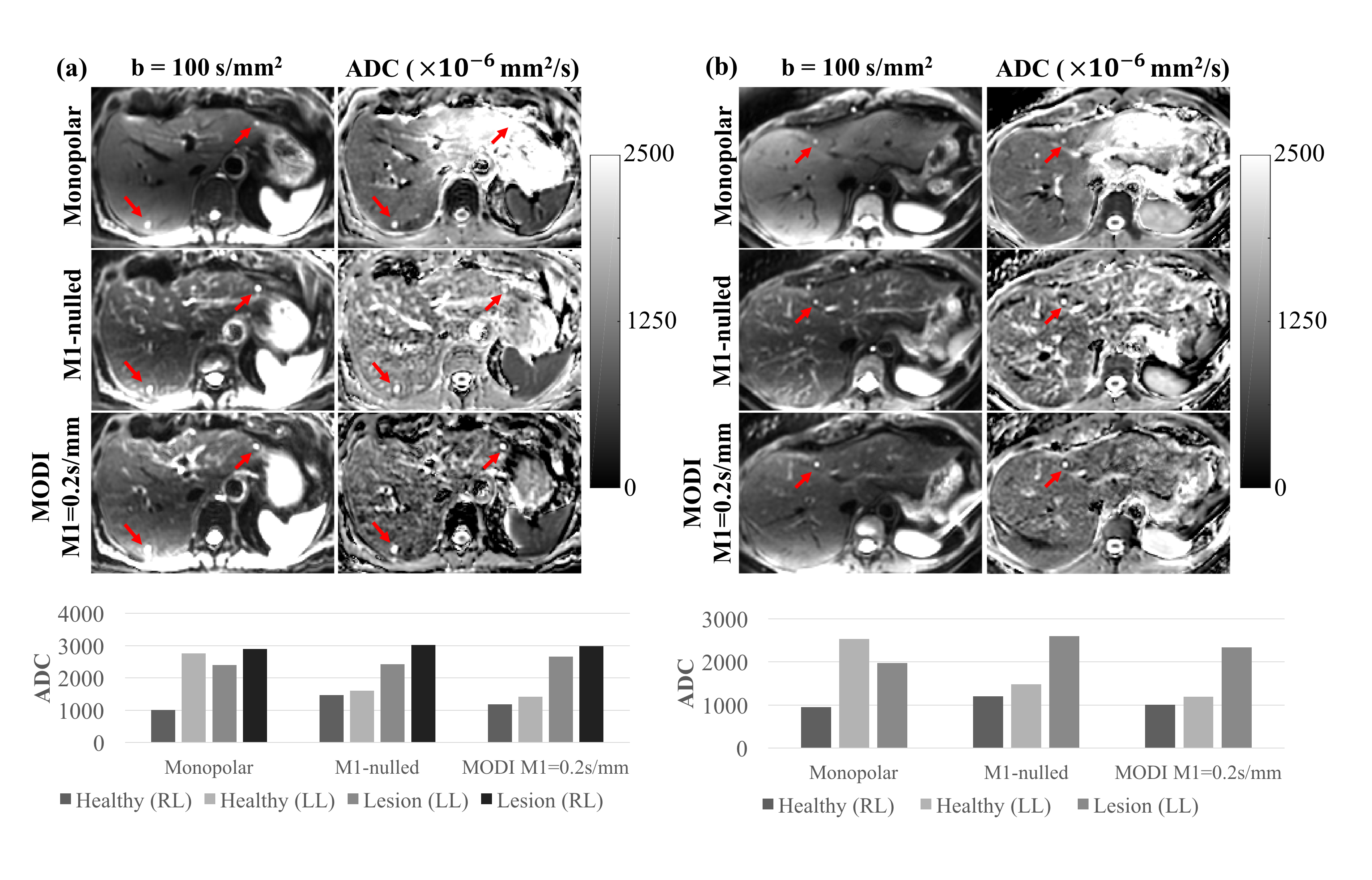
Patient experiments: Five patient volunteers with suspected hepatic lesions were scanned with the same setup as the healthy volunteer study after informed written consent and IRB approval. DW images of the conventional monopolar diffusion waveform, motion-compensated waveform with M1-nulling, and MODI waveform with M1 = 0.2s/mm were acquired under respiratory triggering.
Results
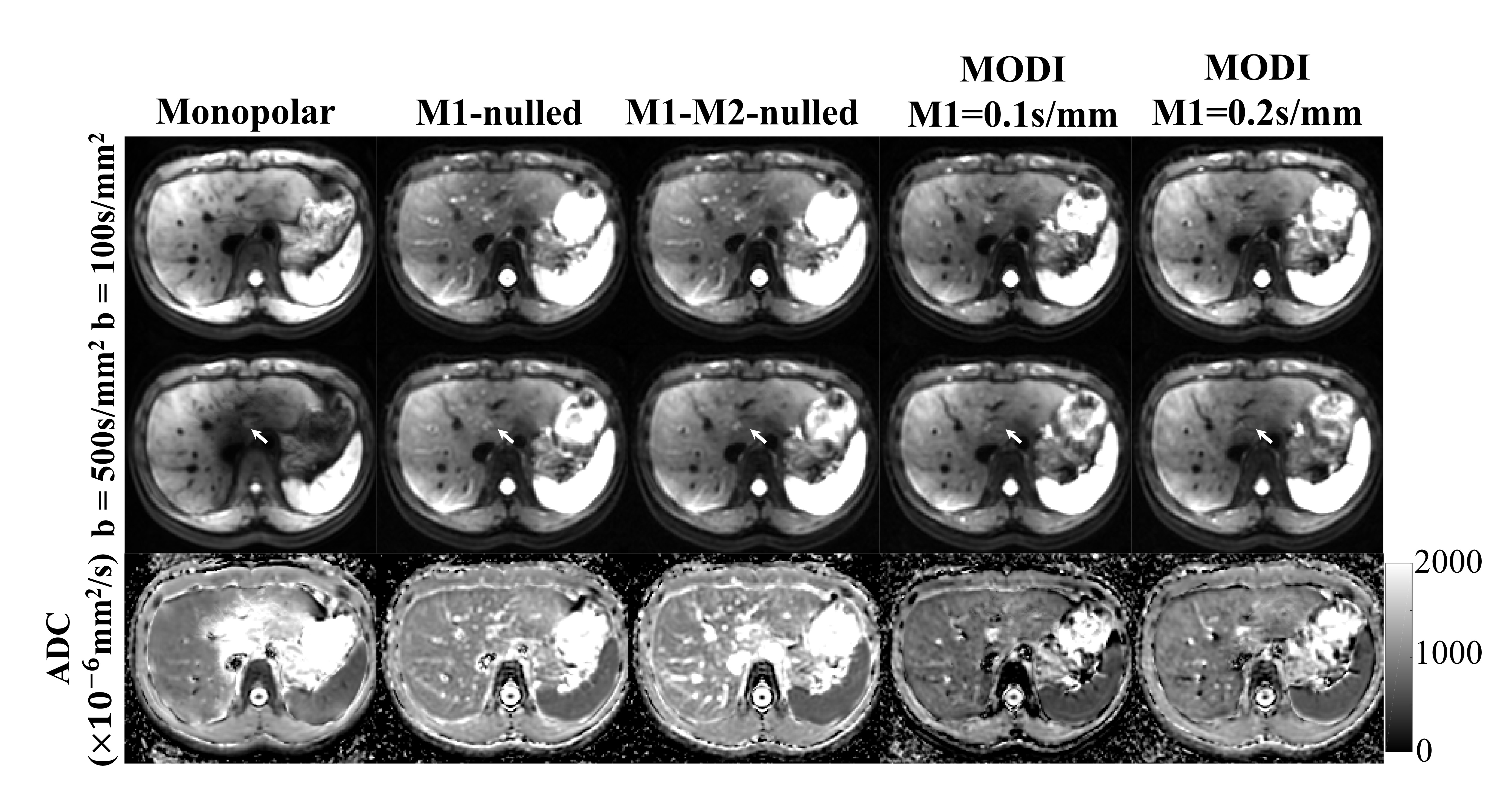
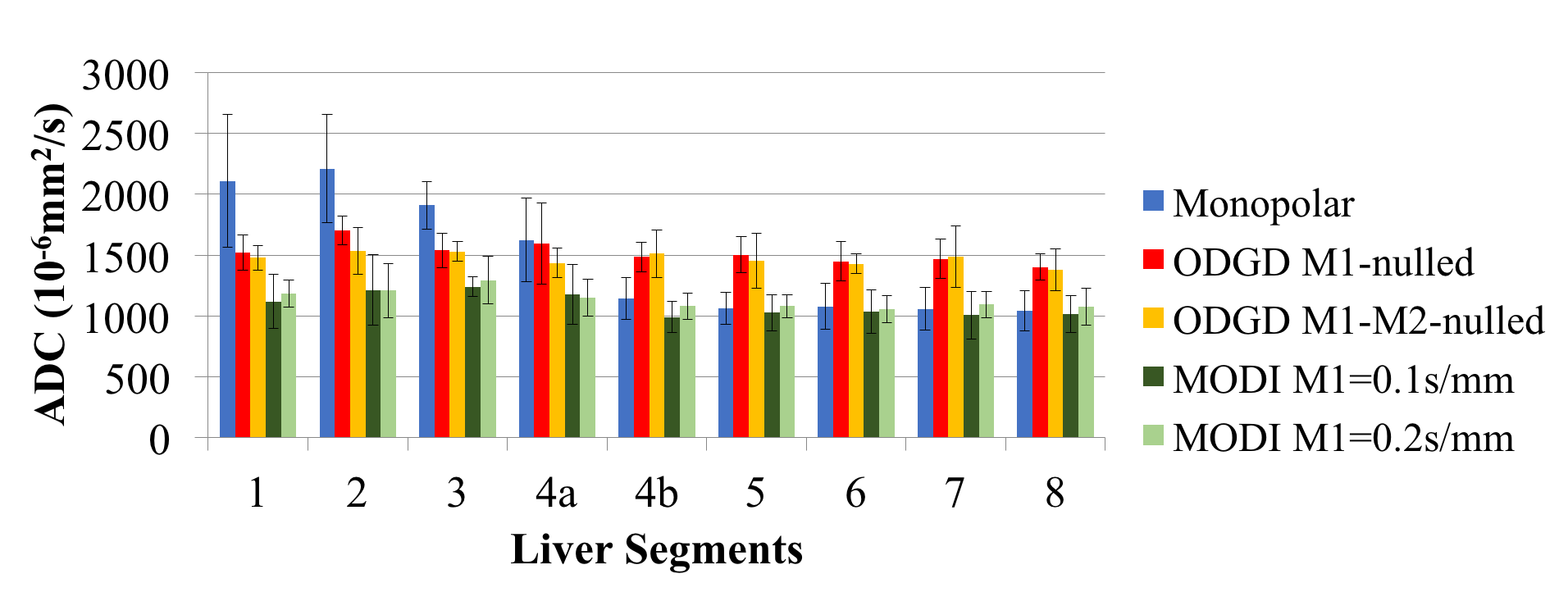
Example DW images as well as ADC maps from one healthy volunteer are shown in Fig.3. Fig.4 presents the average and standard deviation of the ROI measurements of ADC in different liver segments across the healthy volunteers. Two representative patient imaging examples are shown in Fig.5.Discussion
In this study, a M1-Optimized Diffusion Imaging (MODI) method was proposed to acquire motion-robust, blood-suppressed liver DWI with optimized diffusion encoding waveforms. Healthy volunteer experiments and a feasibility evaluation in patients have been performed to investigate the bias of the proposed MODI method.
Compared to the conventional monopolar DWI, MODI is able to provide ADC measurements with reduced bias, particularly in the left lobe of the liver. In contrast to the moment-nulled waveforms5-8, MODI can dephase most of the blood signal but still maintain motion-robustness leading to unbiased ADC maps throughout the liver. Overall, the proposed MODI method is promising for obtaining reliable DW images and quantitative ADC measurements over the entire liver.
Although this work has demonstrated the promise of the proposed moderate M1 approach, the specific choice of M1 value needs to be optimized in future work. MODI also needs to be evaluated in a large number of patients to investigate its performance for lesion detection and characterization throughout the entire liver.
Conclusion
This study has developed and demonstrated the feasibility of a M1-Optimized Diffusion Imaging (MODI) method for the acquisition of motion-robust, blood-suppressed liver DWI.Acknowledgements
The authors would like to acknowledge research support from GE Healthcare.References
[1] Zhou, I.Y., Gao, D.S., Chow, A.M., Fan, S., Cheung, M.M., Ling, C., Liu, X., Cao, P., Guo, H., Man, K. and Wu, E.X., 2014. Effect of diffusion time on liver DWI: An experimental study of normal and fibrotic livers. Magnetic resonance in medicine, 72(5), pp.1389-1396.
[2] Taouli, B., Chouli, M., Martin, A.J., Qayyum, A., Coakley, F.V. and Vilgrain, V., 2008. Chronic hepatitis: role of diffusion‐weighted imaging and diffusion tensor imaging for the diagnosis of liver fibrosis and inflammation. Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine, 28(1), pp.89-95.
[3] Murphy, P., Wolfson, T., Gamst, A., Sirlin, C. and Bydder, M., 2013. Error model for reduction of cardiac and respiratory motion effects in quantitative liver DW‐MRI. Magnetic resonance in medicine, 70(5), pp.1460-1469.
[4] Kwee, T.C., Takahara, T., Niwa, T., Ivancevic, M.K., Herigault, G., Van Cauteren, M. and Luijten, P.R., 2009. Influence of cardiac motion on diffusion-weighted magnetic resonance imaging of the liver. Magnetic Resonance Materials in Physics, Biology and Medicine, 22(5), pp.319-325.
[5] Aliotta, E., Wu, H.H. and Ennis, D.B., 2017. Convex optimized diffusion encoding (CODE) gradient waveforms for minimum echo time and bulk motion–compensated diffusion‐weighted MRI. Magnetic resonance in medicine, 77(2), pp.717-729.
[6] Peña-Nogales, Ó., Zhang, Y., Wang, X., Luis-Garcia, R., Aja-Fernández, S., H Holmes, J. and Hernando, D., 2018. Optimized Diffusion-Weighting Gradient Waveform Design (ODGD) formulation for motion compensation and concomitant gradient nulling. Magnetic resonance in medicine, in press.
[7] Aliotta, E., Moulin, K. and Ennis, D.B., 2018. Eddy current–nulled convex optimized diffusion encoding (EN‐CODE) for distortion‐free diffusion tensor imaging with short echo times. Magnetic resonance in medicine, 79(2), pp.663-672.
[8] Ozaki, M., Inoue, Y., Miyati, T., Hata, H., Mizukami, S., Komi, S., Matsunaga, K. and Woodhams, R., 2013. Motion artifact reduction of diffusion‐weighted MRI of the liver: Use of velocity‐compensated diffusion gradients combined with tetrahedral gradients. Journal of Magnetic Resonance Imaging, 37(1), pp.172-178.
Figures