1791
Dynamic contrast-enhanced MR imaging of hypervascular liver lesions: comparison of conventional breath-hold and a free-breathing acquisition technique with compressed sensing and motion-state-resolved reconstruction1magnetic resonance imaging, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 2Magnetic Resonance Imaging, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, China, 3MR Collaborations, Siemens Healthcare, Ltd., Beijing, China, 4MR-Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
We investigated a prototype free-breathing Cartesian volumetric interpolated breath-hold examination (VIBE) protocol with compressed sensing (CS) and motion-state-resolved reconstruction as extra-dimension (XD-VIBE) for Gd-DTPA-enhanced dynamic liver imaging by comparing it with conventional breath-hold VIBE. We found that it provided good image quality and diagnostic performance for hypervascular liver lesion detection except for the pre-contrast phase. This is a promising option for patients with poor breath-holding capacity.
Introduction/Purpose
Dynamic contrast-enhanced liver imaging is essential for the detection and characterization of liver lesions. However, patients with hearing loss or poor breath-holding capacity (e.g., young children and elderly patients) often cannot follow breath-holding instructions, leading to poor image quality. Therefore, a free-breathing MRI technique is desirable. Recently, a free-breathing Cartesian volumetric interpolated breath-hold examination (VIBE) with compressed sensing (CS) and simultaneous acquisition of a navigation signal for motion-state-resolved reconstruction as extra dimension (XD-VIBE) technique produced good image quality and accurate liver metastatic tumor detection in the portal venous phase (PVP), but low image quality in the arterial phase (AP) compared to the conventional breath-hold (BH) examination (1). Therefore, we investigated the image quality and diagnostic value of this technique for hypervascular liver lesions (HLLs) by comparing it to conventional BH-VIBE.Methods
Twenty-one patients (18 men, 3 women; age range, 33 - 75 years) with 40 HLLs (mean diameter, 24.3 mm; range, 6 - 108 mm) underwent MRI examination on a 3T MR system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). Free-breathing XD-VIBE image data was acquired during gadopentetate dimeglumine (Gd-DTPA; Bayer Schering Pharma, Berlin, Germany) injection (TE/TR = 1.4/4.3 ms; FOV = 380×320 mm2; matrix = 320×240; flip angle = 10°; slice thickness = 3.0 mm, acquisition time ~174 seconds) along with a self-navigation signal. All patients had either prior (seven with benign lesions/metastases) or subsequent BH-VIBE exams performed 3 - 5 days afterwards (fourteen patients with suspected HCC). A single arterial phase was obtained using BH-VIBE with an acquisition time of 16 s and sharing consistent acquisition parameters with XD-VIBE.
The continuous XD-VIBE data were grouped in 19 subsequent time increments with a 9.4 s temporal resolution, with each isolated phase resolved into six motion states using the self-navigation signal. Images were reconstructed inline by an adapted scanner reconstruction pipeline, taking ten minutes. After a truth reader selected four-phase images matched with BH-VIBE from XD-VIBE, all VIBE data were randomly presented to three independent blinded reviewers to score image quality on a 5-point scale, higher scores indicating a better exam. Eight weeks later, the three readers independently assessed the presence of HLLs greater than 5 mm in size and scored lesion conspicuity on the same scale. In the last session, both imaging sets were directly compared to evaluate the major signs, including arterial hyperenhancement (APHE), washout and/or capsule/pseudo-capsule on PVP and/or the delayed phase (DP) (2) for 22 proven hepatocellular carcinomas (HCCs), without the readers knowing the sequence type.
For the statistical analysis, the intraclass correlation coefficient (ICC), Friedman test with post-hoc test, Wilcoxon signed-rank test, and McNemar's test were performed.
Results
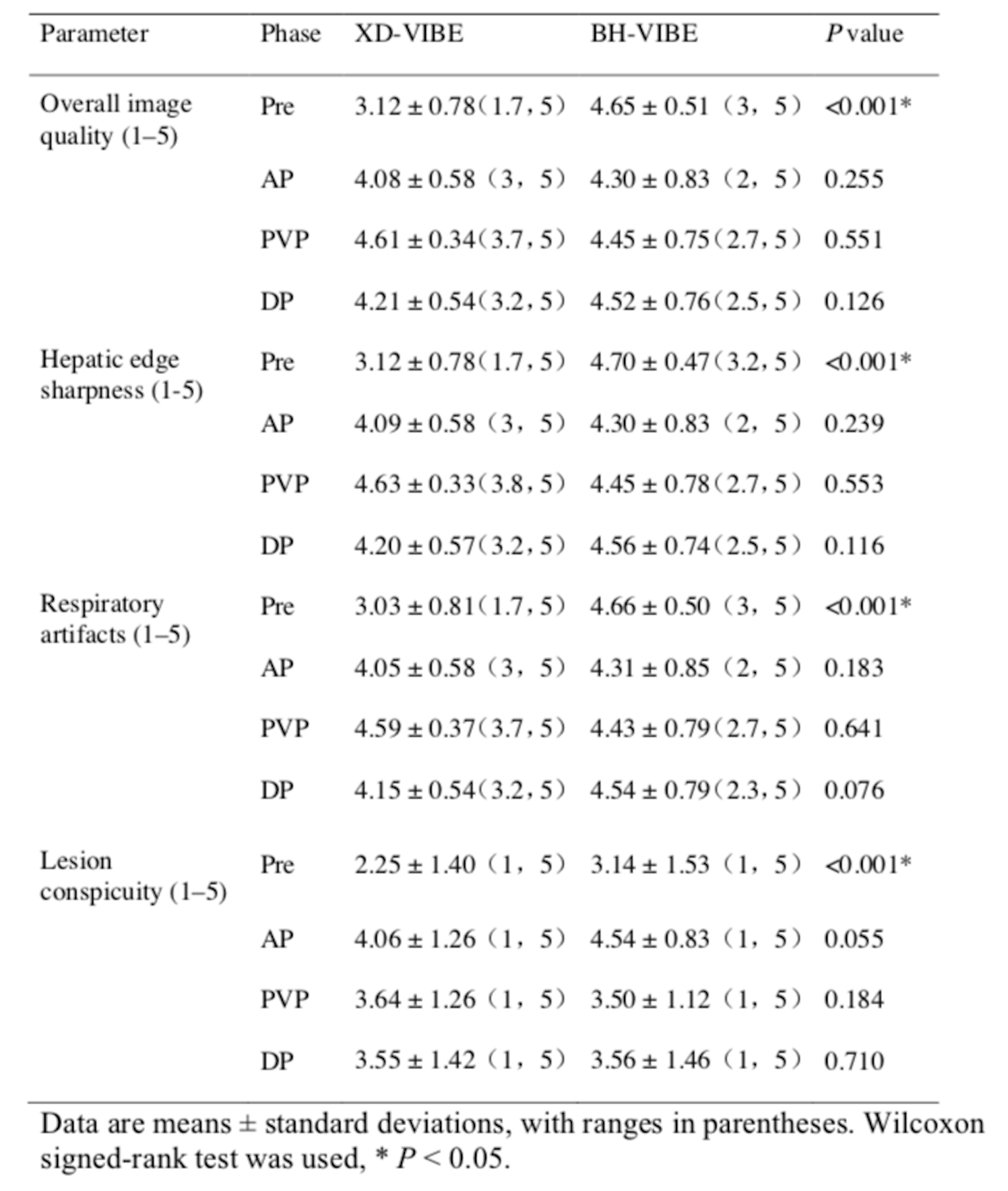
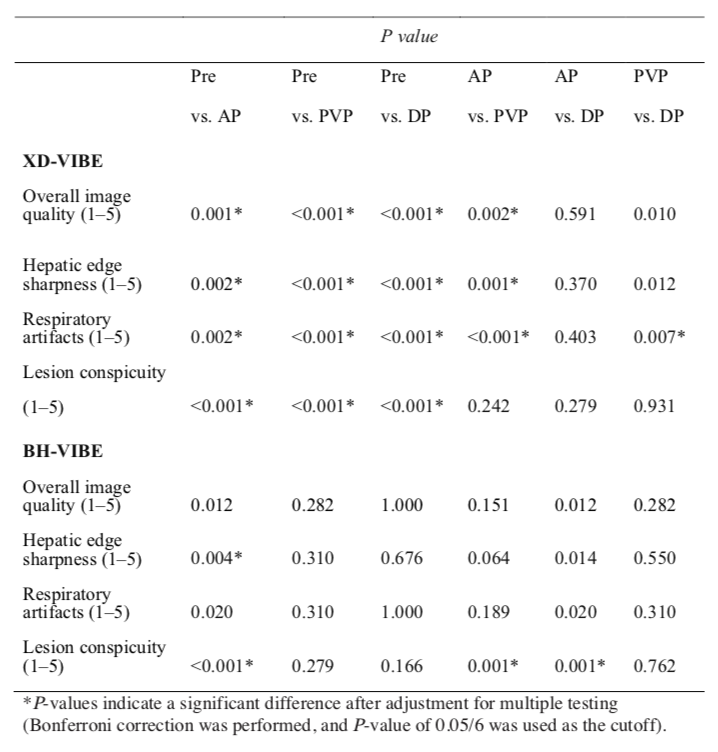
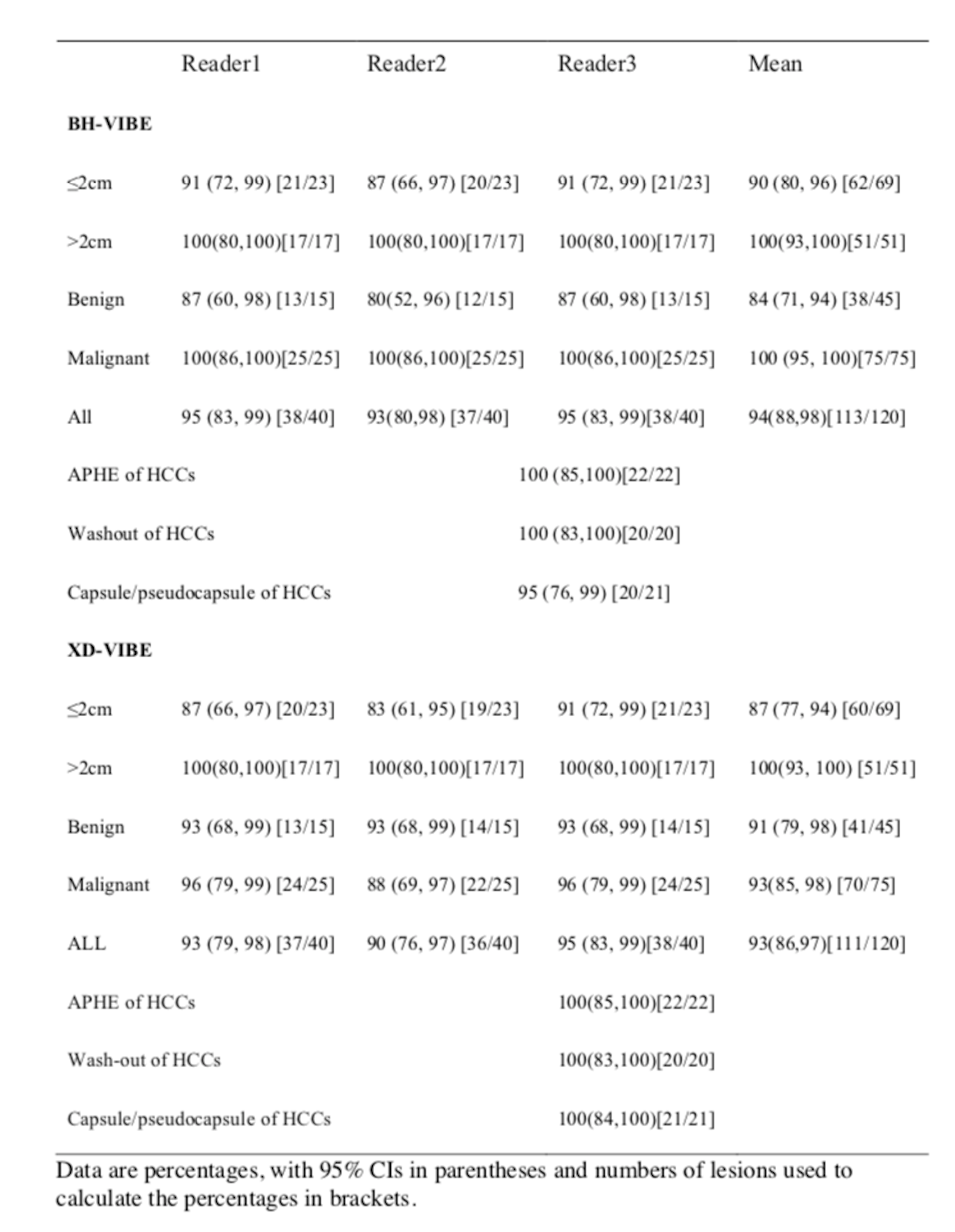
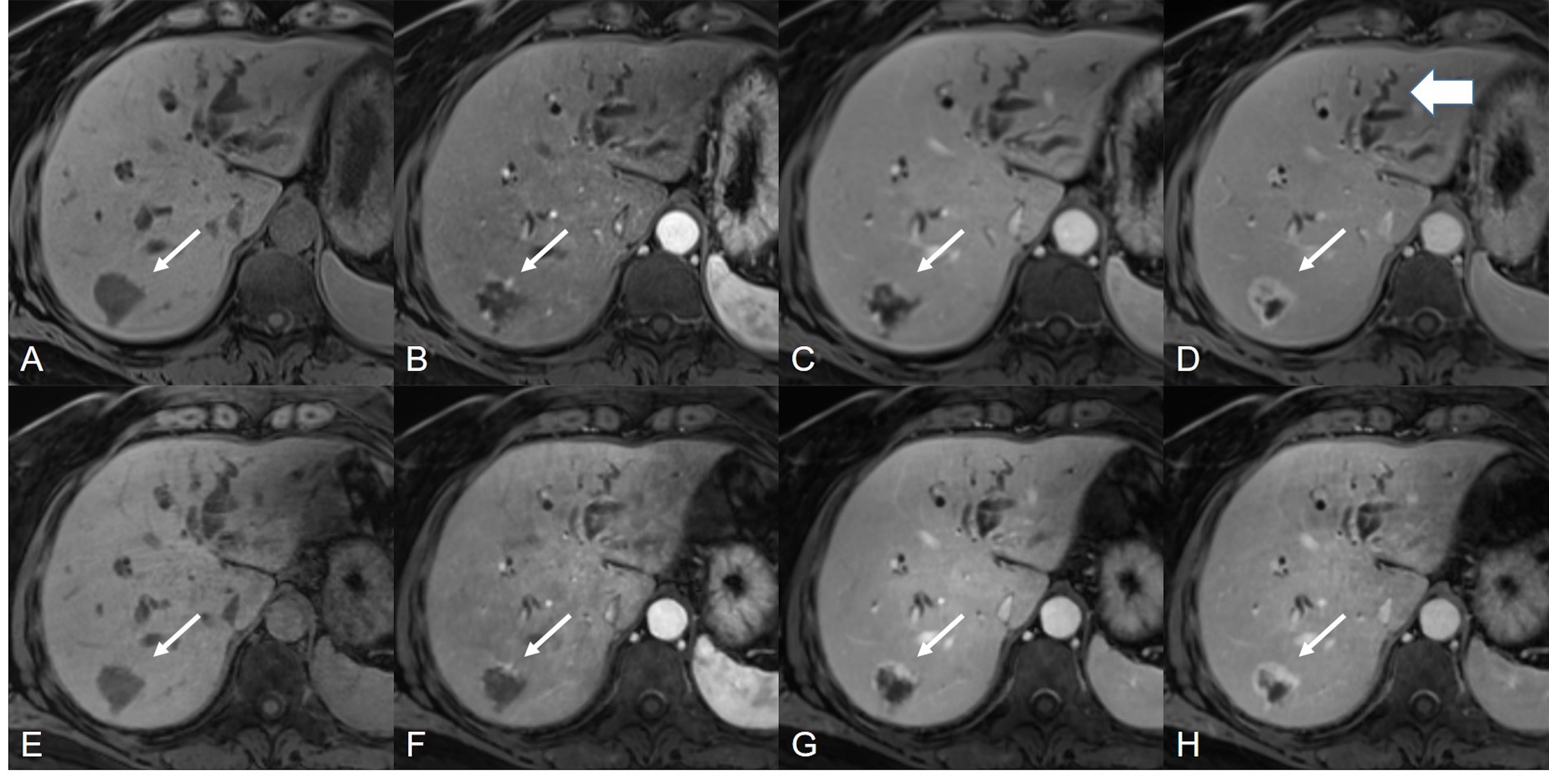
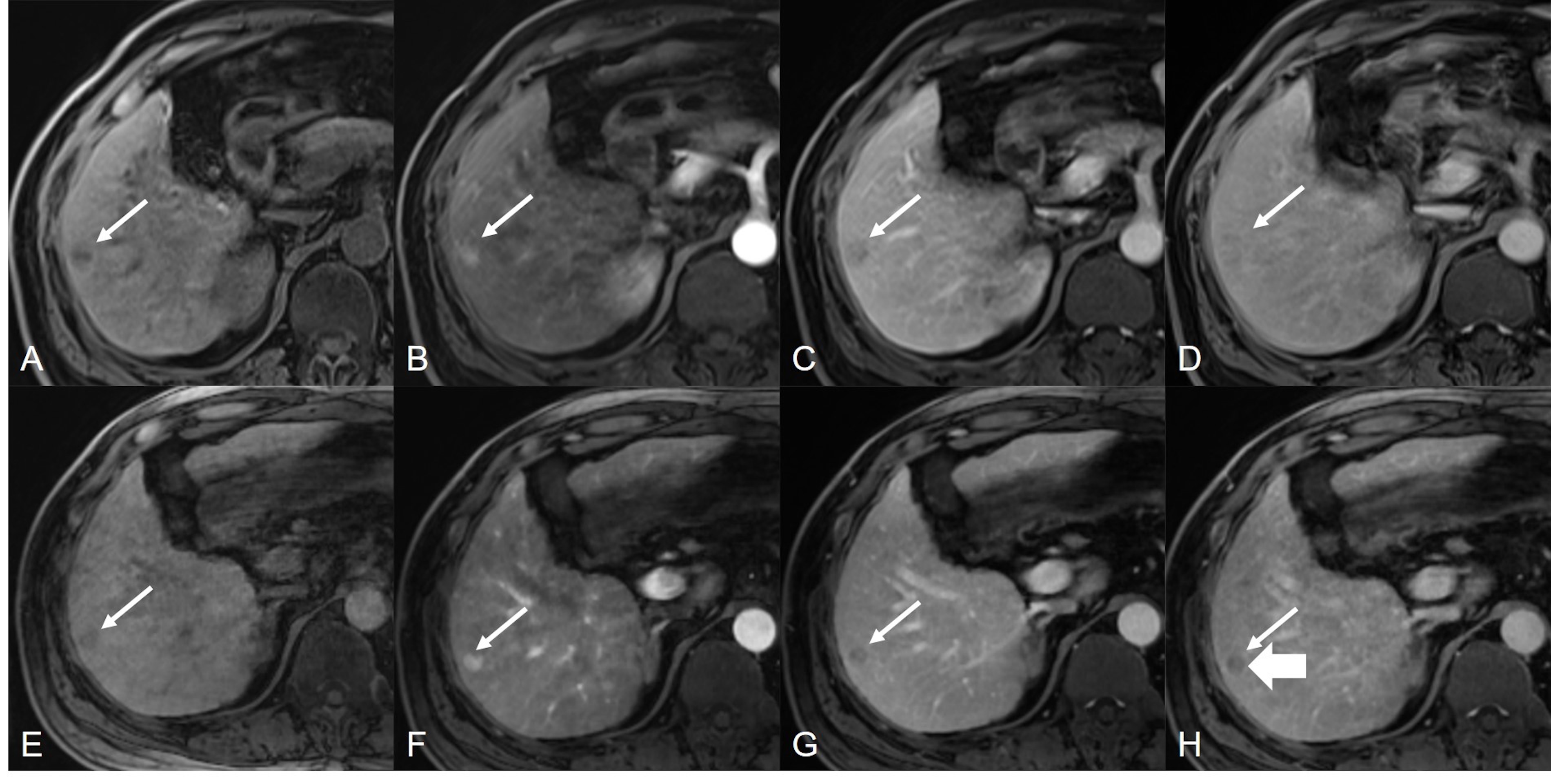
Motion state 1 of 6 showed the best image quality and was selected for subsequent image analysis. The ICCs were fair to excellent for all items. The optimal late AP was determined by a truth reader at the fourth contrast-enhanced time point in 90.4% (33.3 seconds) and the third in 4.8% (23.6 seconds) of cases on XD-VIBE. One patient (4.8%) had “early AP” on XD-VIBE and was deemed a suboptimal AP. There was no significant difference in image quality and lesion conspicuity for AP, PVP, and DP (all P > 0.05) between XD-VIBE and BH-VIBE, except for the pre-contrast phase (P< 0.05) (Table 1). For XD-VIBE, the pre-contrast phase demonstrated significantly lower scores overall compared with the other three phases (all P < 0.05), and PVP showed the best image quality (all P < 0.05) but similar HLL conspicuity compared to AP or DP (both P > 0.05) (Table 2). For diagnostic performance, XD-VIBE and BH-VIBE were comparably capable of detecting HLLs (Figure 1), regardless of tumor size/type, as well as major signs of HCC (Figure 2) (all P > 0.05) (Table 3).Discussion
We used Cartesian trajectories to enable faster reconstruction of the high-dimensional dataset and combined a motion-state-resolved reconstruction without specific motion model, advantageous for reducing motion-induced blurring. XD-VIBE had good motion robustness compared to BH-VIBE, except for the pre-contrast phase. In two patients unable to breath-hold, XD-VIBE outperformed BH-VIBE in image quality and HLL detection. The results from a previous study were slightly different (1), possibly because our sample size was smaller. The poor quality of pre-contrast images for XD-VIBE might be because the so-called “pre-contrast” was scanned during contrast injection, which could cause inhomogeneity of the navigation signal.Conclusion
The proposed free-breathing dynamic contrast-enhanced liver imaging protocol XD-VIBE provided comparable image quality and HLL detection to BH-VIBE on post-contrast phases. It holds promise for meeting the diagnostic requirements of patients with compromised breath-holding capability.Acknowledgements
No acknowledgement found.References
1. Kaltenbach B, Bucher AM, Wichmann JL, Nickel D, Polkowski C, Hammerstingl R, et al. Dynamic Liver Magnetic Resonance Imaging in Free-Breathing: Feasibility of a Cartesian T1-Weighted Acquisition Technique With Compressed Sensing and Additional Self-Navigation Signal for Hard-Gated and Motion-Resolved Reconstruction. Investigative radiology. 2017;52(11):708-14.
2. Tang A, Bashir MR, Corwin MT, Cruite I, Dietrich CF, Do RKG, et al. Evidence Supporting LI-RADS Major Features for CT- and MR Imaging-based Diagnosis of Hepatocellular Carcinoma: A Systematic Review. Radiology. 2018;286(1):29-48.
Figures