1789
Interface Analysis of the Liver and Focal Hepatic Lesions in Hepatobiliary Phase Imaging: A Comparison between Free-breathing Radial and Conventional Breath-hold Acquisition Technique.1Department of Radiology, Gifu University, Gifu, Japan, 2Department of Radiology services, Gifu University, Gifu, Japan
Synopsis
The free-breathing radial k-space sampling technique is especially useful for patients with limited breath-holding capacity in liver MR imaging, however, its degradation of spatial resolution in the plane compared with the Cartesian sampling is the greatest disadvantage. We assessed the fat-suppressed three-dimensional T1-weighted fast field echo imaging with pseudo-golden-angle radial stack-of-stars sampling technique with gate and track (3D-VANE) compared with the conventional breath-hold Cartesian sampling (BH-eTHRIVE) in hepatobiliary phase imaging. Our results demonstrated that 3D-VANE with thinner effective slice thickness (thin-slice 3D-VANE) achieved comparable interface resolution, less artifact and better image quality compared with BH-eTHRIVE.
Introduction
The hepatobiliary phase imaging is especially excellent for the differentiation between lesions with and without functional hepatocytes and now widely used in clinical imaging 1. The hepatobiliary phase imaging is commonly performed approximately 20-second-single breath-hold sequence using fat-suppressed three-dimentional gradient echo T1-weighted imaging (e.g. eTHRIVE; enhanced T1 high resolution isotropic volume excitation) 2, which is still challenging for patients such as young children or critically ill adults, resulting in degradation of image quality.
The free-breathing radial k-space sampling (FBRS) technique has been applied in liver MR imaging, which is useful for patients with limited breath-holding capacity 3-5. However, its degradation of spatial resolution in the plane compared with the breath-hold Cartesian sampling is the greatest disadvantage 3,6. We hypothesized that the improved effective slice thickness in the FBRS was a solution of this disadvantage. The purpose of this study was to compare the interface resolution of the liver and focal hepatic lesions on hepatobiliary phase imaging between the FBRS and conventional breath-hold Cartesian sampling technique.
Materials and Methods
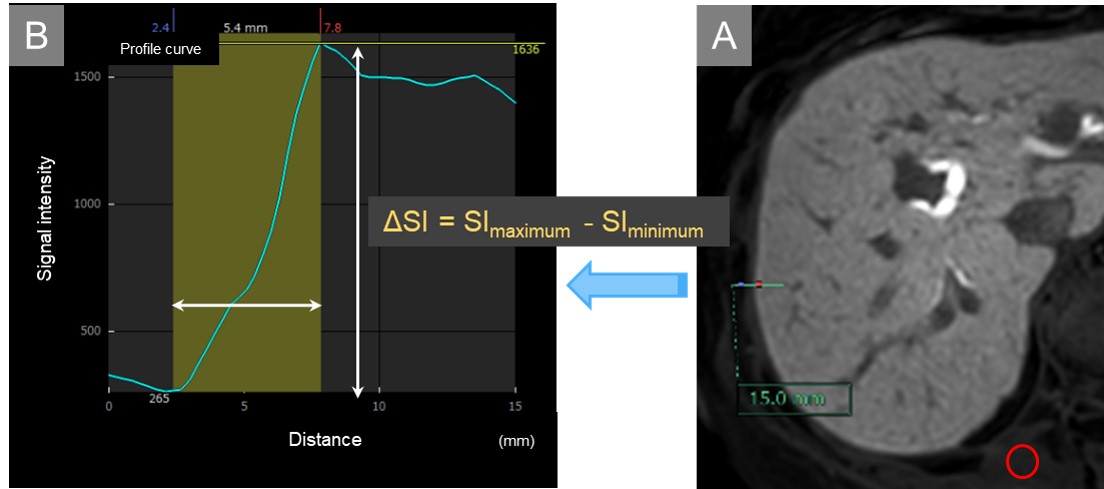
Institutional review board approval was obtained for this prospective HIPAA-compliant study. Gadoxetic acid-enhanced hepatobiliary phase imaging with three acquisition sets was performed in 66 patients (39 men, 27 women; mean age, 66.8 years, range, 27-84 years). Image acquisition sets included breath-hold fat-suppressed three-dimensional T1-weighted fast field echo imaging (3D-FFE T1WI/FS) with the Cartesian sampling technique (BH-eTHRIVE; slice thickness/gap, 4/-2 mm; acquisition time, 16.8 sec), free-breathing 3D-FFE T1WI/FS with pseudo-golden-angle radial stack-of-stars sampling with gate and track (3D-VANE; 4/-2 mm; 160.3 sec), and 3D-VANE with thinner effective slice thickness (thin-slice 3D-VANE; 2/0 mm; 256.6 sec) at a 3-T clinical scanner (Ingenia CX; Philips Healthcare, Netherlands) with a 32-channel phased-array receiver coil. The hepatobiliary phase images were obtained 19 min (range, 15-26 min) after an intravenous bolus injection of gadoxetic acid and these acquisition sets were performed in random order. Continuous signal intensities (SIs) were recorded from extra-hepatic to intra-hepatic parenchyma or from hepatic parenchyma to hypointense nodule, respectively, using commercially available workstation (SYNAPSE VINCENT; FUJIFILM Corporation, Tokyo, Japan) (Fig. 1). For quantitative image analyses, the relative rate of SIs change (ΔSI) (RRC) was calculated as ΔSI/ distance/ SImuscle in the right hepatic robe (RRCR), left hepatic robe (RRCL), and 101 hypointense nodules (RRCN; mean maximum diameter, 15.9 mm, range, 4-68 mm). In addition, for subgroup analyses, RRCs in the hypointense nodules in maximum diameter of greater than 10 mm (RRCN > 10mm; 23.0 mm, 11-68 mm) and 10 mm or less (RRCN ≤ 10mm; 7.3 mm, 4-10 mm) were also evaluated. For qualitative image analyses, a radiologist graded sharpness of the liver and hypointense nodule, homogeneity of liver parenchyma, motion artifact, and overall image quality using a five-point rating scale. Quantitative measurements and qualitative scales were compared between three sequences using repeated measures ANOVA/ pairwise t-test with Bonferroni correction (BC) and Friedman test with pairwise Wilcoxson signed rank test with BC, respectively.Results
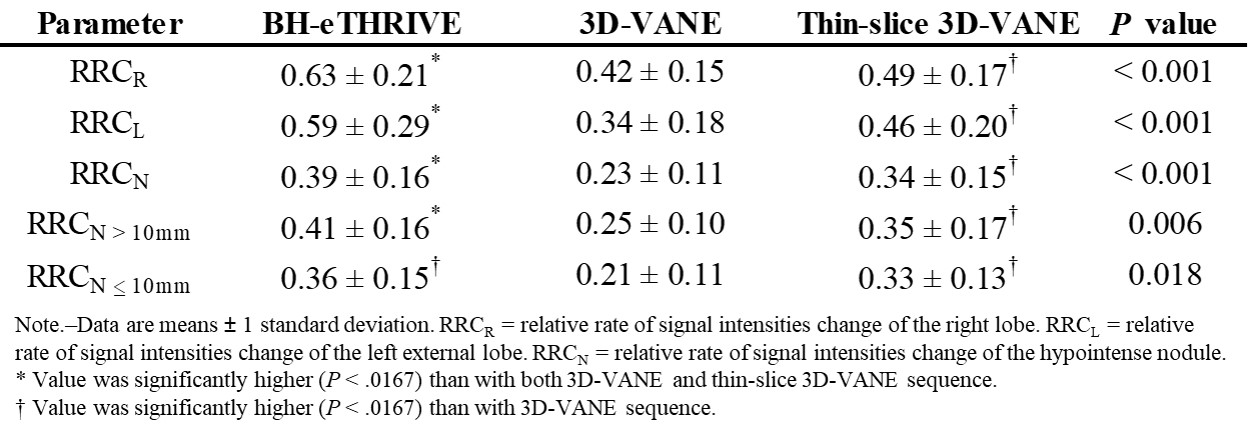
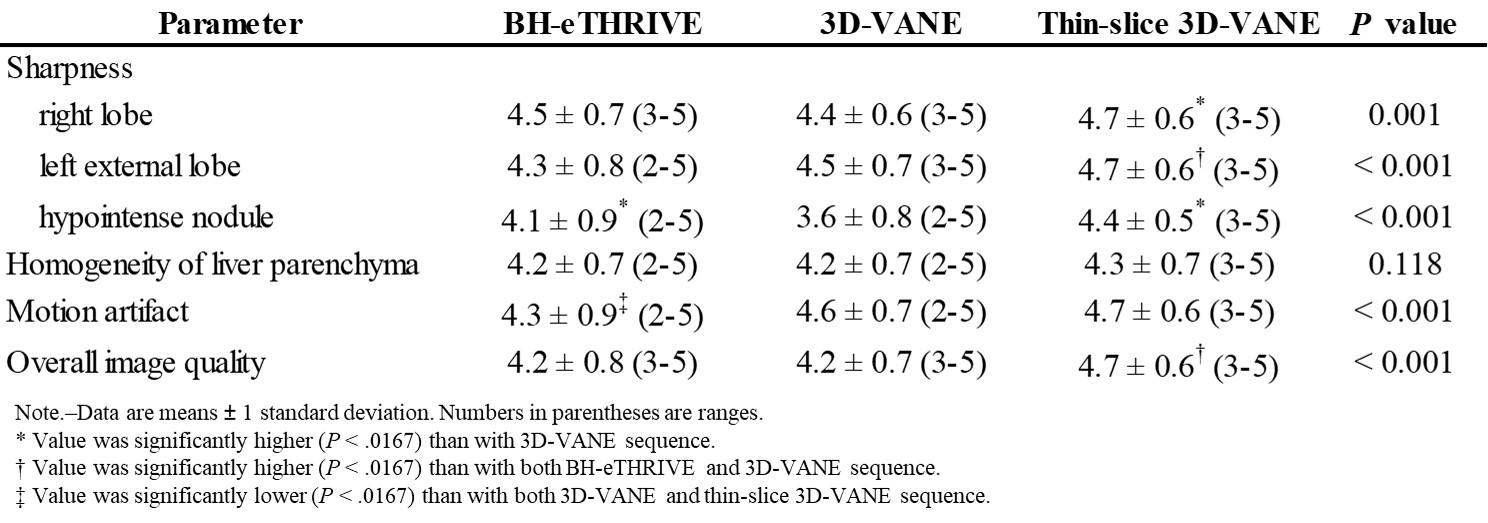
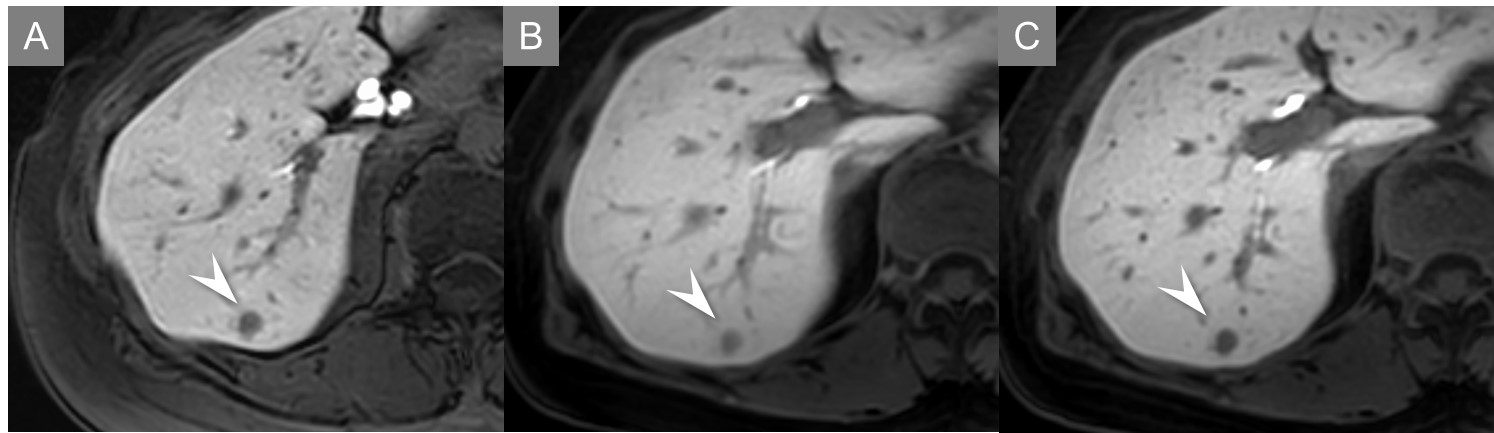
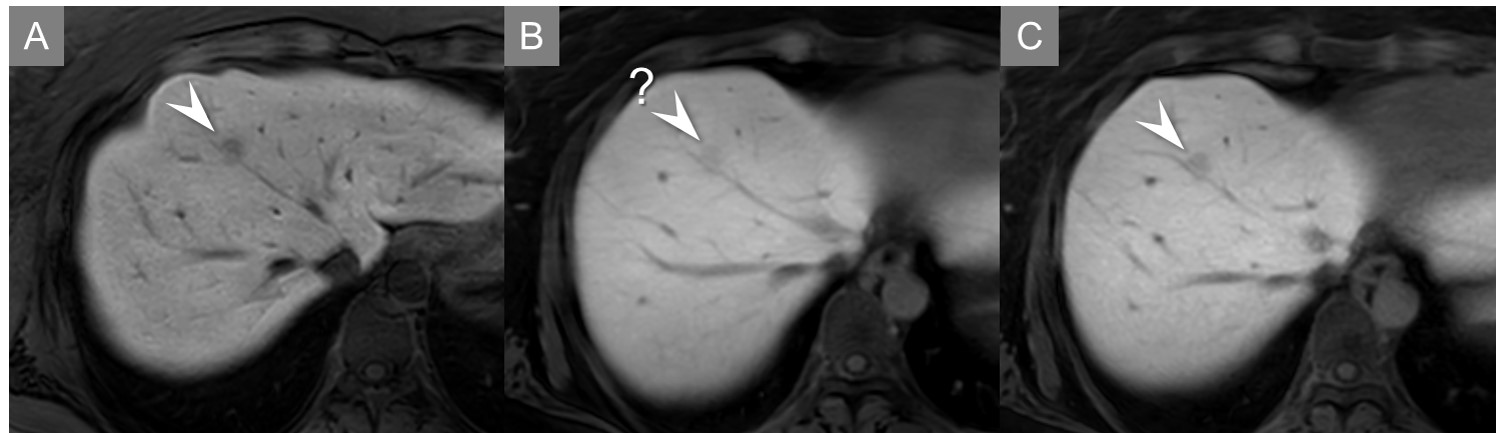
Quantitative results were demonstrated in Table 1. RRCR, RRCL, and RRCN was significantly higher in the order corresponding to BH-eTHRIVE (0.63, 0.59, 0.39), thin-slice 3D-VANE (0.49, 0.46, 0.34), and 3D-VANE (0.42, 0.34, 0.23) (P ≤ 0.024). RRCN ≤ 10mm was comparable between thin-slice 3D-VANE (0.33) and BH-eTHRIVE (0.36). Qualitative results were demonstrated in Table 2. Sharpness of hypointense nodule was comparable between thin-slice 3D-VANE (4.4) and BH-eTHRIVE (4.1) (Fig. 2-3). Motion artifact and overall image quality with thin-slice 3D-VANE (4.7, 4.7) were significantly better than with BH-eTHRIVE (4.3, 4.2) (P < 0.001).Discussion
RRCs with BH-eTHRIVE were significantly higher than with both 3D-VANE sequences. The Cartesian sampling technique fills peripheral portion of the k-space, which affect spatial resolution, more fully than the radial sampling 2.
Motion artifact with both 3D-VANE sequences was significantly improved compared with BH-eTHRIVE. In addition, sharpness of left external lobe with thin-slice 3D-VANE was significantly better than with BH-eTHRIVE. Visualization of hypointense nodule was comparable between thin-slice 3D-VANE and BH-eTHRIVE. The FBRS technique is motion-robust data acquisition, which has a motion-averaging effect and prevents the appearance of ghosting artifacts depending on breathing or cardiac pulsation 7. Thinner effective slice thickness in thin-slice 3D-VANE contributes to the high spatial resolution of structures.
Conclusion
The interface resolution of the liver and focal hepatic lesions were comparable between thin-slice 3D-VANE and BH-eTHRIVE. Thin-slice 3D-VANE demonstrated less motion artifact and better image quality compared with BH-eTHRIVE.Acknowledgements
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.References
- Sano K, Ichikawa T, Motosugi U, et al. Imaging study of early hepatocellular carcinoma: usefulness of gadoxetic acid-enhanced MR imaging. Radiology 2011;261:834-44.
- Goshima S, Noda Y, Kajita K, et al. Gadoxetic acid-enhanced high temporal-resolution hepatic arterial-phase imaging with view-sharing technique: Impact on the LI-RADS category. European journal of radiology 2017.
- Chandarana H, Block TK, Rosenkrantz AB, et al. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Investigative radiology 2011;46:648-53.
- Azevedo RM, de Campos RO, Ramalho M, Heredia V, Dale BM, Semelka RC. Free-breathing 3D T1-weighted gradient-echo sequence with radial data sampling in abdominal MRI: preliminary observations. AJR American journal of roentgenology 2011;197:650-7.
- Reiner CS, Neville AM, Nazeer HK, et al. Contrast-enhanced free-breathing 3D T1-weighted gradient-echo sequence for hepatobiliary MRI in patients with breath-holding difficulties. European radiology 2013;23:3087-93.
- Kajita K, Goshima S, Noda Y, et al. Thin-slice Free-breathing Pseudo-golden-angle Radial Stack-of-stars with Gating and Tracking T1-weighted Acquisition: An Efficient Gadoxetic Acid-enhanced Hepatobiliary-phase Imaging Alternative for Patients with Unstable Breath Holding. Magnetic resonance in medical sciences : MRMS : an official journal of Japan Society of Magnetic Resonance in Medicine 2018.
- Weiss J, Taron J, Othman AE, et al. Feasibility of self-gated isotropic radial late-phase MR imaging of the liver. European radiology 2017;27:985-94.
Figures