1788
Breath hold free hepatobiliary phase imaging: usefulness of stack-of-stars acquisition1Department of Radiology, University of Yamanashi, Chuo-shi, Japan, 2Department of Diagnostic Radiology and Neuroradiology, University Medicine Greifswald, Greifswald, Germany, 3MR Collaboration and Development, GE Healthcare, Tokyo, Japan, 4MR Collaboration and Development, GE Healthcare, Madison, WI, United States, 5MR Engineering, GE Healthcare, Waukesha, WI, United States
Synopsis
We compared the quality of hepatobiliary phase (HBP) imaging using the prototype pulse sequences stack-of-stars liver acquisition with volume acceleration (LAVA) (LAVA Star) with or without navigator echoes (LAVA Starnavi+ and LAVA Starnavi-) and Cartesian LAVA with navigator echoes (Cartesian LAVAnavi+). LAVA Starnavi+ showed better image quality, liver edge sharpness, and hepatic vein clarify than others. The images of LAVA Starnavi+ had less streak artifacts than those of LAVA Starnavi- The use of both stack-of-stars acquisition and navigator echo is the best solution to obtain HBP images without breath hold in terms of quality of images.
Introduction
Postcontrast magnetic resonance (MR) image of the liver is typically obtained with breath hold 3D gradient echo sequence. However, breath hold for >10 seconds is sometimes difficult in some patients. While respiratory gating with navigator echoes is commonly used to obtain 3D gradient echo sequence without breath hold, stack-of-stars technique is supposed to be robust for respiratory motion compared with Cartesian sampling (1). Up to now, it has not been systematically investigated which breath hold free technique is more effective for hepatobiliary phase (HBP) imaging. Thus, the aim of this study was to compare the quality of HBP imaging using the prototype pulse sequences stack-of-stars liver acquisition with volume acceleration (LAVA) (LAVA Star) with or without navigator (LAVA Starnavi+ and LAVA Starnavi-) and Cartesian LAVA with navigator (Cartesian LAVAnavi+).Methods
This retrospective study was approved by the institutional review board; the requirement for informed patient consent was waived. Seventy-two patients (male: female, 39: 33; mean age, 68.0 ± 10.0 years) who underwent gadoxetic acid enhanced MRI with a 3-T MRI system were enrolled. Thirty HCCs (10 early HCCs and 20 hypervascular HCCs; mean size, 10.3 ± 6.6 [range, 5–35] mm) were observed in 18 patients. Fifteen minutes after injection of gadoxetic acid, 4 different LAVA acquisitions were performed as following order: Cartesian LAVAnavi+, LAVA Starnavi+, Cartesian breath hold LAVA, and LAVA Starnavi-. Three breath hold free LAVA sequences (Cartesian LAVAnavi+, LAVA Starnavi-, and LAVA Starnavi+) were used for evaluation in this study. Acquisition time of those three sequences are as follows; Cartesian LAVAnavi+, about 3 min; LAVA Starnavi-, 1min and LAVA Starnavi+, about 4 min. Two radiologists performed a visual assessment of overall image quality, liver edge sharpness, hepatic vein clarity, streak artifact, and respiratory motion/pulsation artifact using a 5-point scale for each 3 sequences. Quantitative evaluation was performed by calculating the signal intensity ratios of the liver-to-spleen, liver-to-lesion, and liver-to-portal vein (PV). Intergroup comparisons were performed between 3 sequences. Kappa coefficients (κ) and intraclass correlation coefficients (r) were calculated to determine interobserver agreement. Sharpness of images were evaluated by comparing full width at half maximum (FWHM) of the line spread function.Results
LAVA Starnavi+ showed better image quality, liver edge sharpness, and hepatic vein clarify than others (P < 0.0001–0.0183) (Fig. 1). Cartesian LAVAnavi+ also showed better image quality than LAVA Starnavi- (P = 0.0015) (Figs. 1a and 2). Focused on the poor breath hold cases, LAVA Starnavi+ showed better image quality than LAVA Starnavi- (P = 0.0234). No significant difference was observed between Cartesian LAVAnavi+ and LAVA Starnavi- (P = 1.0000) or LAVA Starnavi+ (P = 0.2824) (Figs. 1b and 3). LAVA Starnavi- showed the lowest image quality (P < 0.0001). The images of LAVA Starnavi+ had less streak artifacts than those of LAVA Starnavi- (P < 0.0001), while no streak artifact in Cartesian LAVAnavi+. The images of Cartesian LAVAnavi+ had stronger respiratory motion/pulsation artifact than others (P < 0.0001) (Fig. 4). The liver-to-spleen ratio of LAVA Starnavi- was higher than others (P < 0.0001–0.0015). The liver-to-lesion and liver-to-PV ratios of Cartesian LAVAnavi+ were lower than others (P < 0.0001–0.0012) (Fig. 5). Interobserver agreement were good to excellent in all evaluation (κ = 0.660–0.873 and r = 0.630–0.875). LAVA Starnavi- (mean, 4.80 ± 1.70) showed higher FWHM (= higher blurring) than Cartesian LAVAnavi+ (3.77 ± 0.75) and LAVA Starnavi+ (3.73 ± 0.83) (P = 0.0003–0.0009).Discussion
Our results revealed that combination of stack-of-stars acquisition and navigator echoes (LAVA Starnavi+) was better than those of the acquisitions with only navigator echoes or starck-of-stars technique. Stack-of-stars acquisition without navigator echoes (LAVA Starnavi-) showed lower image quality than Cartesian acquisition with navigator echoes (LAVAnavi+), indicating that stack-of-stars acquisition itself cannot suppress the respiratory motion artifact as navigator echoes. Therefore, both stack-of-stars acquisition and navigator echoes are needed for obtaining high quality HBP images without breath hold. Signal intensity ratio of liver-to-spleen of LAVA Starnavi- was higher than that of Cartesian LAVAnavi+ and LAVA Starnavi+. This result suggested that the T1 contrast can decrease due to navigator echoes. In the navigator technique, the longitudinal magnetization recovers during waiting time of navigator triggering. This causes T1 contrast decrease and SI of the objects increase (2).Conclusion
The use of both stack-of-stars acquisition and navigator echo is the best solution to obtain HBP images without breath hold in terms of quality of images.Acknowledgements
No acknowledgement found.References
(1) Peters DC, Korosec FR, Grist TM, et al. Undersampled projection reconstruction applied to MR angiography. Magn Reson Med. 2000;43(1):91-101.
(2) Fujiwara Y, Maruyama H, Kosaka N, et al. Simultaneous acquisition of high-contrast and quantitative liver T1 images using 3D phase-sensitive inversion recovery: a feasibility study. Acta Radiol. 2017;58(8):899-905.
Figures

Stacked bar graph representing results of the visual assessment for the parameters of image quality.
(a) The image quality of LAVA Starnavi+ was better than Cartesian LAVAnavi+ and LAVA Starnavi- Cartesian LAVAnavi+ also showed better image quality than LAVA Starnavi-.
(b) Focused on the cases with poor breath hold, LAVA Starnavi+ showed better image quality than LAVA Starnavi-.
(c) The score for liver edge sharpness of LAVA Starnavi+ was better than Cartesian LAVAnavi+ and LAVA Starnavi-
(d) The score for hepatic vein clarity of LAVA Starnavi+ was better than Cartesian LAVAnavi+ and LAVA Starnavi-.

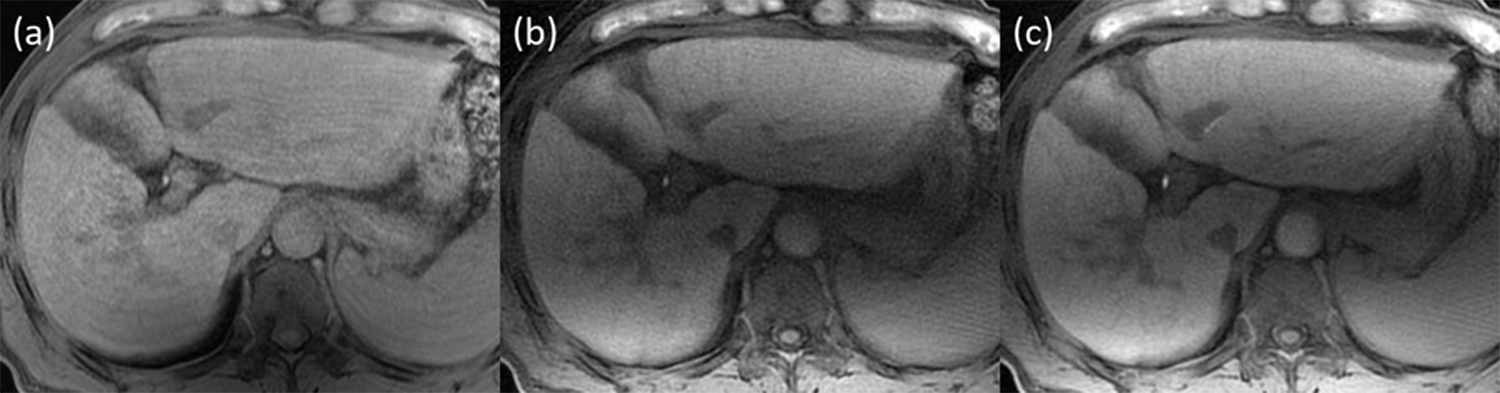
Comparison of images of the 3 sequences (good breath hold case).
(a) Cartesian LAVAnavi+, (b) LAVA Starnavi-, (c) LAVA Starnavi+
These are the images of a 62-year-old woman with good breath hold. In this case, Cartesian LAVAnavi+ and LAVA Starnavi+ showed similar image quality. The image quality of LAVA Starnavi- was lower than others, however severe artifact was not observed.
Comparison of images of the 3 sequences (poor breath hold case).
(a) Cartesian LAVAnavi+, (b) LAVA Starnavi-, (c) LAVA Starnavi+
These are the images of a 65-year-old man with poor breath hold. In this case, Cartesian LAVAnavi+ image showed respiratory motion artifact, however, motion artifact was not observed in the LAVA Star sequences regardless of with or without navigator. The image quality of LAVA Starnavi+ was the best in this case. It is assumed that LAVA Star sequence is less likely to be affected by respiratory motion.

Stacked bar graph representing results of the visual assessment for the parameters of artifacts.
(a) Streak artifact was observed only on the images of LAVA Star sequences. The images of LAVA Starnavi+ had less streak artifacts than those of LAVA Starnavi-.
(b) The images of Cartesian LAVAnavi+ had stronger respiratory motion/pulsation artifact than those of LAVA Starnavi- and LAVA Starnavi+.
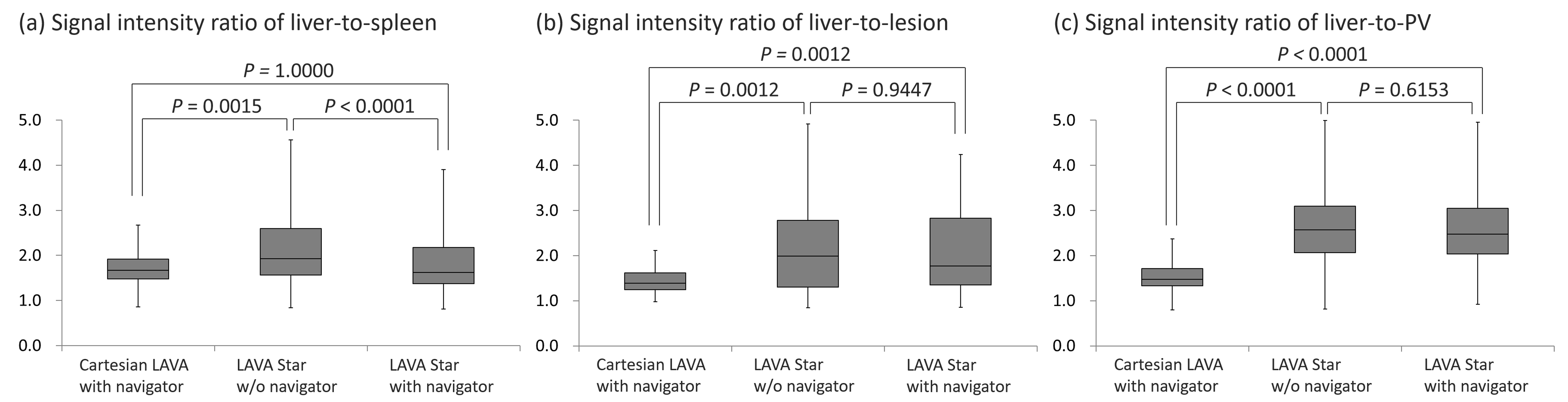
Box plots of the signal intensity ratios of liver-to-spleen (SIRliver/spleen, (a)), liver-to-lesion (SIRliver/lesion (b)), and liver-to-portal vein (SIRliver/lesion (c)).
(a) SIRliver/spleen of LAVA Starnavi- was higher than that of Cartesian LAVAnavi+ and LAVA Starnavi+.
(b) SIRliver/lesion of Cartesian LAVAnavi+ was lower than that of LAVA Starnavi- and LAVA Starnavi+.
(c) SIRliver/lesion of Cartesian LAVAnavi+ was also lower than that of LAVA Starnavi- and LAVA Starnavi+.