1786
Artifacts in the arterial phase during gadoxetic-acid-enhanced MRI: multiple arterial phases versus single arterial phase from two different vendors1Tianjin First Center Hospital, Tianjin, China, 2MR Collaboration, Siemens Healthcare, Beijing, China
Synopsis
In this article, we compare the usefulness of multiple arterial phases (APs) and a relatively short breath-hold single AP to reduce the motion artifact in gadoxetic-acid-enhanced MRI. The transient motion artifact (TMA) score and phase timing of the AP in 540 consecutive patients were retrospectively analyzed. Our results showed that the best mean TMA score for multiple APs was significantly lower than that for the conventional single AP, but a relatively short breath-hold single AP did not reduce the incidence of TMA. In addition, multiple APs can capture more satisfactory ones, which meets clinical diagnostic requirements.
Objectives
Gadoxetic-acid-enhanced MRI is widely used in clinical practice to quantify liver tumors [1]. However, motion artifacts that appear during the arterial phase (AP) can reduce image quality. In this article, we aimed to compare the usefulness of multiple APs and a single, relatively short breath-hold AP of gadoxetic-acid-enhanced MRI to reduce transient motion artifact (TMA) in the AP.Methods
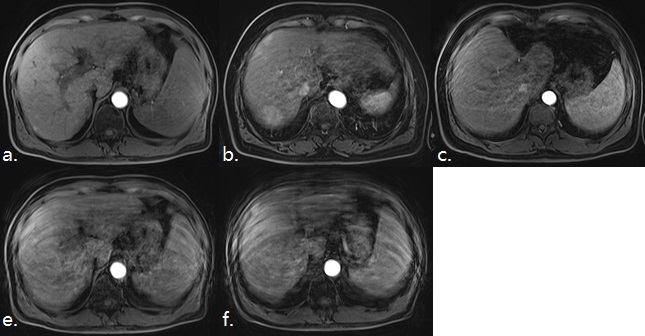
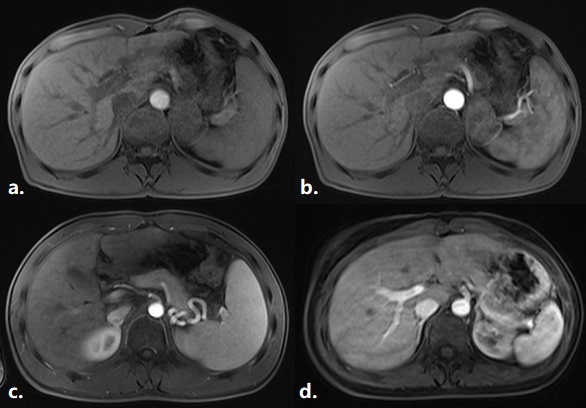
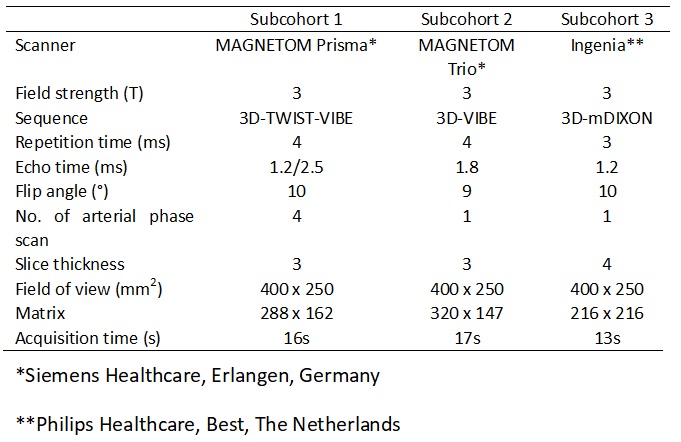
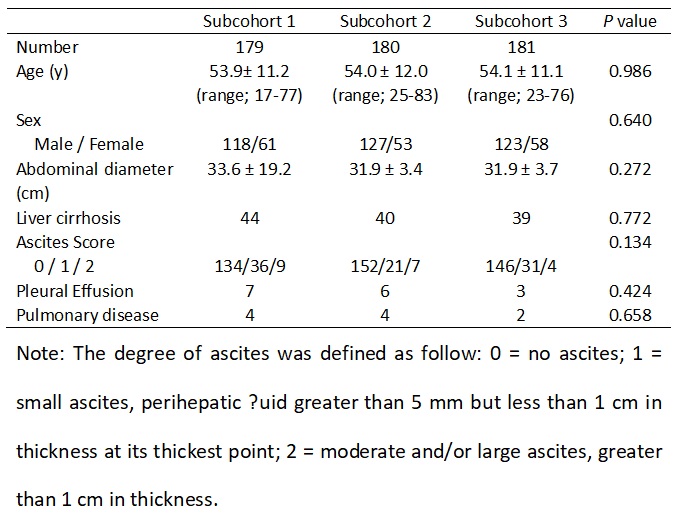
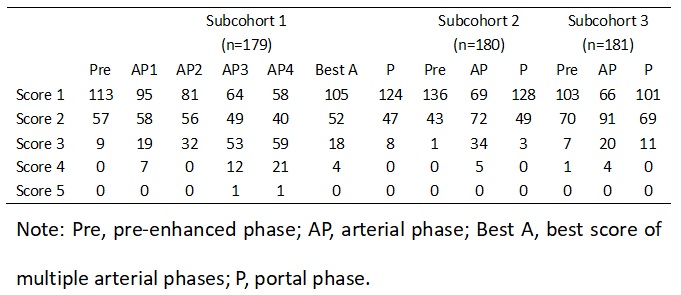
In this retrospective study, 540 consecutively enrolled patients underwent gadoxetic-acid-enhanced MRI at our center. They underwent quadruple APs (subcohort 1, n = 179) or a single AP from two different vendors, either a single AP with 17 s breath-hold (subcohort 2, n = 180) or 13 s breath-hold (subcohort 3, n = 181). The MR parameters are shown in Table 1. The baseline patient characteristics were recorded, including age, sex, abdominal diameter (maximal transverse diameter measured from the coronal images), liver cirrhosis, ascites [3], pleural effusion, and history of lung disease. The degree of TMA in the pre-enhanced AP (each AP in subcohort 1) and portal phase images were scored using a 5-point scale [3] (Figure 1). The phase timing of the AP was also assessed using a 4-point scale [3] (Figure 2). The patients’ baseline characteristics, TMA score, and frequency of acquisition of an early and/or adequate late AP were compared among the subcohorts.Results
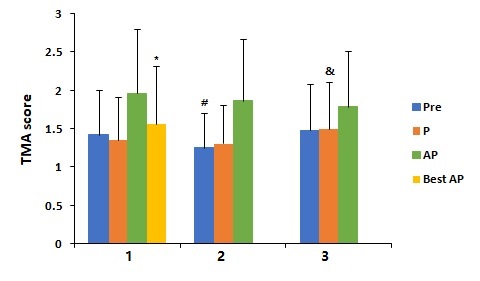
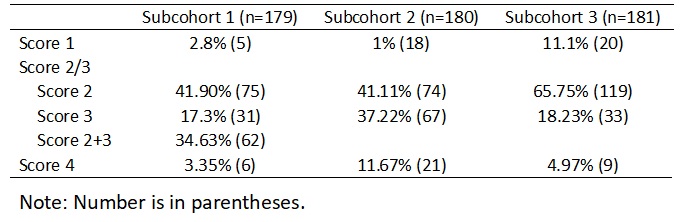
The characteristics of all the subcohorts are shown in Table 2. There were no differences among the three subcohorts (P > 0.05). The artifact scores are summarized in Table 3 and Figure 3. For the artifact score of the pre-enhanced images, only one patient in subcohort 1 showed a severe artifact (score 4), and subcohort 2 was significantly lower than subcohorts 1 (P = 0.023) and 3 (P < 0.001). For the artifact score of the AP, 15.6% (28/179), 2.8% (5/180), and 2.2% (4/181) patients showed a severe artifact in subcohorts 1, 2, and 3, respectively. The artifact score increased gradually from AP1 to AP4 (1.65 ± 0.82, 1.84 ± 0.91, 2.09 ± 0.98, 2.25 ± 1.06) in subcohort 1. There was no significant difference between the mean artifact score of the quadruple AP in subcohort 1 and single AP in subcohorts 2 and 3 (P = 0.138). The best mean score of the quadruple APs in subcohort 1 was better than those for subcohort 2 (P = 0.002) and 3 (P < 0.001), and only 2.2% (4/179) of patients showed a severe artifact. For the artifact score of the portal phase, no patient showed any severe artifact, and subcohort 3 was significantly higher than subcohorts 1 (P = 0.023) and 2 (P = 0.004). The distribution of phase timing in the arterial phase is shown in Table 4.Discussion and Conclusion
Our results showed that the mean TMA score of pre-enhanced and portal-phase images was different among the three groups. This may be due to the pulse sequence design varying among different vendors. The mean TMA score of multiple APs was similar to that for a single AP, but the best mean TMA score for multiple APs was better than that for a single AP. This finding was consistent with previous studies [2-5] and presents the ability of multiple APs to mitigate the TMA of the AP in gadoxetic-acid-enhanced MRI. In our study, shortening the breath-hold time of a single AP by 4 s did not reduce the incidence of TMA. Therefore, within a certain range, the breath-hold duration which was closely related to respiratory artifacts had no effect on the TMA score. In our study, the frequency of acquisition of early and/or adequate late AP was higher with multiple APs. This was also consistent with a previous study [5] and presents the ability of multiple APs to capture a satisfactory AP which meet the clinical diagnostic needs. However, shortening the breath-hold time of a single AP by 4 s decreased the frequency of acquisition of an adequate late AP. This suggests that the time to start scanning of the AP should be delayed appropriately, when the breath-hold time has been shortened.Acknowledgements
NoReferences
1. Huppertz A, Balzer T, Blakeborough A, et al. Improved detection of focal liver lesions at MR imaging: multicenter comparison of gadoxetic acid-enhanced MR images with intraoperative findings. Radiology, 2004;230(1):266-275.
2. Pietryga JA, Burke LM, Marin D, et al. Respiratory Motion artifact affecting hepatic arterial Phase imaging with gadoxetate Disodium: Examination Recovery with a Multiple Arterial Phase Acquisition. Radiology, 2014;271(2):426-434.
3. Xiao YD, Ma C, Liu J, et al. Transient severe motion during arterial phase in patients with Gadoxetic acid administration: Can a five hepatic arterial subphases technique mitigate the artifact? Exp Ther Med, 2018;15:3133-3139.
4. Yoon JH, Lee JM, Yu MH, et al. Triple Arterial Phase MR Imaging with Gadoxetic Acid Using a Combination of Contrast Enhanced Time Robust Angiography, Keyhole, and View sharing Techniques and Two-Dimensional Parallel Imaging in Comparison with Conventional Single Arterial Phase. Korean J Radiol, 2016;17(4): 522-532.
5. Min JH, Kim YK, Kang TW, et al. Artifacts during the arterial phase of gadoxetate disodium-enhanced MRI: Multiple arterial phases using view-sharing from two different vendors versus single arterial phase imaging. Eur Radiol, 2018;28(8):3335-3346.
Figures