1783
Better Depiction of Cystic Duct with Breath-hold 3D MRCP accelerated with GRASE as compared with FSE-based MRCP with Compressed Sensing at 1.5T1Seirei Mikatahara General Hospital, Hamamatsu, Japan, 2Nagoya University, Graduate School of Medicine, Nagoya, Japan, 3Philips Japan, Ltd, Tokyo, Japan, 4Hamamatsu Univ. Hospital, Hamamatsu, Japan
Synopsis
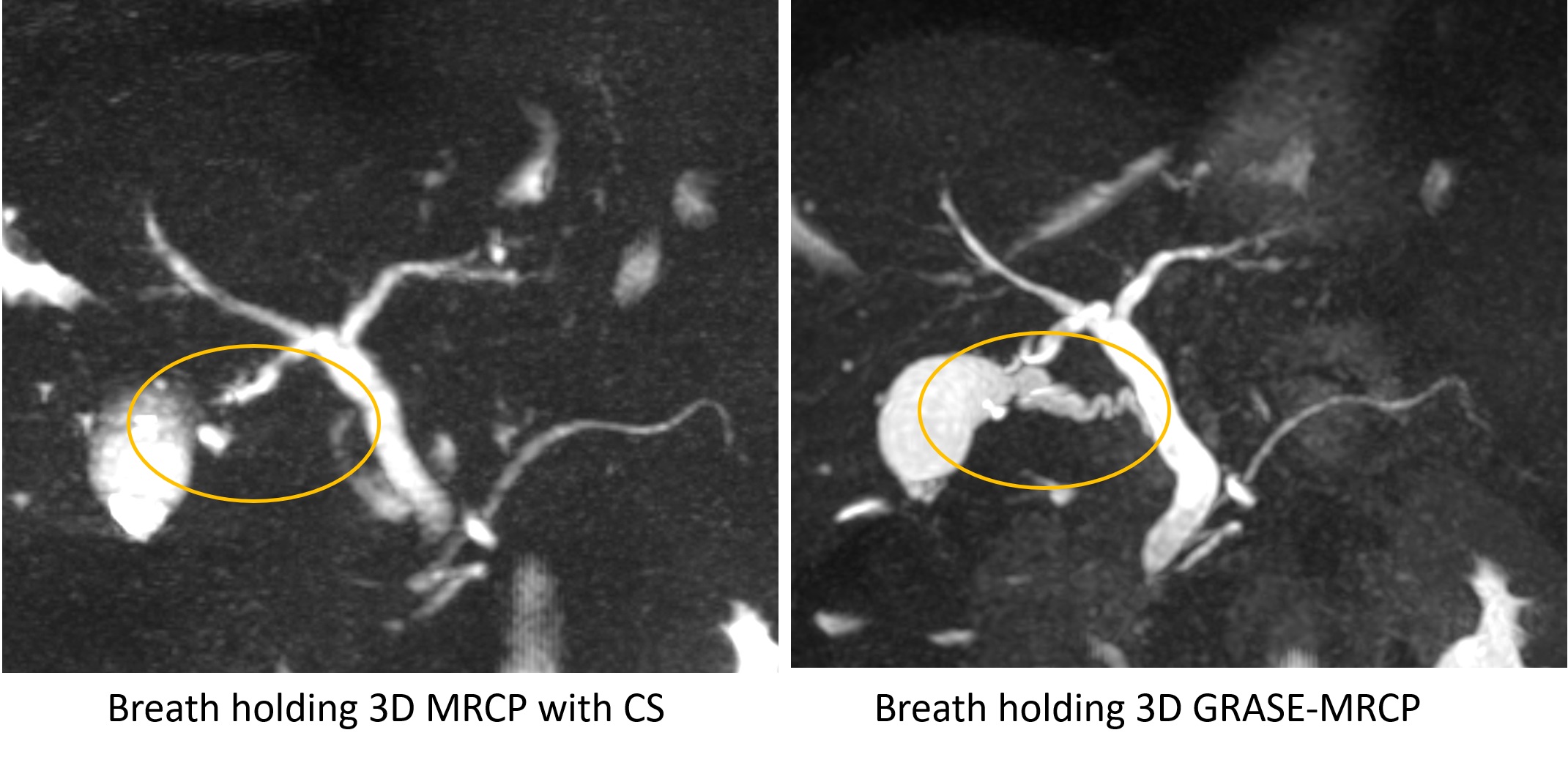
We compared the depiction of the cystic duct between two types of 3D breath-holding MRCP accelerated with GRASE (GRASE-MRCP) and FSE with compressed sensing (CS-MRCP) at 1.5T. Although imaging time and overall image quality
INTRODUCTION
Cholecystectomy is one of the frequent surgical operations. Nowadays laparoscopic cholecystectomy is an established procedure for benign gallbladder lesions. Although the type of cystic duct insertion is one of the most important information before laparoscopic cholecystectomy, conventional MRCP has not constantly delineated the cystic duct because of T1&T2 shortening of the concentrated bile. Previous investigators have reported that the breath-hold FSE-based MRCP accelerated with compressed sensing (CS) performed better, or comparable to conventional respiratory triggered FSE-based MRCP without CS. 1-2 Gradient and spin echo (GRASE) is a hybrid sequence incorporating gradient echoes with EPI readouts to fast spin echo (FSE), which has recently been implemented to 3D MRCP as one of the accelerated options enabling breath-hold MRCP. There are few reports concerning directly comparison between breath-hold CS-MRCP and breath-hold GRASE-MRCP. 3, 4 In this report, we compared the depiction of the biliary trees between two types of 3D breath-holding MRCP accelerated with GRASE (GRASE-MRCP) and FSE with CS (CS-MRCP).METHODS
Thirteen consecutive patients suspected of having pancreatic or biliary disease were recruited. The patient population included 9 males and 4 females with age ranging from 41 – 80 (median age of 70). All patients provided written informed consent. All study was performed on 1.5T MR scanner (Prodiva 1.5T CX, Phillips) with torso array coil. CS-MRCP was operated with TR/TE/FA = 2131/700/90, slice thickness of 1.8mm (- 0.9mm gap) and CS factor of 10. 3. GRASE MRCP utilized TR/TE/FA =330/102/90, slice thickness of 2.4mm (- 1.2mm gap) and EPI factor of 7. Fat saturated axial T1 weighted image (fs T1WI) was performed to measure the signal of the cystic duct on T1WI for reference. The image quality of the overall biliary trees was rated by 4-point scale. (1, poor; 2, fair; 3, good; and 4, excellent) The degree of background suppression was also assessed. The depictions of cystic ducts were rated by 4-point scale. (1, no visualization; 2, <50% visualization; 3, incomplete but ≧ 50% visualization; 4, complete visualization ) Separately, the relative contrasts (RC) of the cystic ducts were measured on fs T1WI. For statistical analysis, the paired t-test, the Wilcoxon signed rank test and the Spearman's rank correlation coefficient were used. Values of p < 0.05 were considered statistically significant.RESULTS
The scan time for CS-MRCP was 20.5 s and 19.7s for GRASE-MRCP. The overall image quality was 3.54 +/- 0.52 for CS-MRCP vs. 3.64 +/- 0.51 for GRASE-MRCP (p=0.697). Background suppression was 3.62 +/- 0.51 vs. 3.00 +/- 0.41 (p=0.004). The depiction of the cystic duct was 3.23 +/- 0.73 vs. 3.85 +/- 0.38 (p = 0.014). The complete visualization (Score 4) of the cystic duct was 5 out of 13 cases (38.5%) on CS-MRCP, and 12 cases (92.3%) on GRASE-MRCP. The rates of cystic duct delineation and the RC of the cystic duct on fsT1WI were inversely correlated in CS-MRCP (r=-0.62; p=0.023), and not significant in GRASE-MRCP (r= -0.17; p=0.577).DISCUSSION
On CS-MRCP images, the depiction of cystic duct showing high signal on fsT1WI became poor. This trend was considered as follows. Concentrated bile in the gallbladder and the cystic duct had shortened both T2 values and T1 values, so that the signal intensity on conventional FSEbased MRCP with long TE became much weak. GRASE-MRCP, on the other side, was less susceptible to the effect of shortening of the T2 values, because its TE was not too long.CONCLUSION
Although overall image quality was the same, breath-hold MRCP accelerated with GRASE better depicted the cystic ducts than FSE with CS probably because its depiction with GRASE was less affected by the T2 shortening effect by the concentrated bile.Acknowledgements
No acknowledgement found.References
1. Zhu L, Wu X, Sun Z, et al. Compressed-Sensing Accelerated 3-Dimensional Magnetic Resonance Cholangiopancreatography: Application in Suspected Pancreatic Diseases. Invest Radiol. 2018 Mar;53(3):150-157.
2. Yoon JH1, Lee SM, Kang HJ, et al. Clinical Feasibility of 3-Dimensional Magnetic Resonance Cholangiopancreatography Using Compressed Sensing: Comparison of Image Quality and Diagnostic Performance. Invest Radiol. 2017 Oct;52(10):612-619.
3. Nam JG, Lee JM, Kang HJ, et al. GRASE Revisited: breath-hold three-dimensional (3D) magnetic resonance cholangiopancreatography using a Gradient and Spin Echo (GRASE) technique at 3T. Eur Radiol. 2018 Sep;28(9):3721-3728.
4. Yoshida M, Nakaura T, Inoue T, Tanoue S, et al. Magnetic resonance cholangiopancreatography with GRASE sequence at 3.0T: does it improve image quality and acquisition time as compared with 3D TSE? Eur Radiol. 2018 Jun;28(6):2436-2443.
Figures