1782
Super high temporal frame rate reconstruction in abdominal dynamic contrast-enhanced MRI using stack-of-stars acquisition (LAVA-Star) under free breathing toward comprehensive hemodynamic analysis of the abdominal vessels and organs: a feasibility studyTetsuya Wakayama1, Daiki Tamada2, Kang Wang3, Ty Cashen3, Ali Ersoz4, Shintaro Ichikawa2, Hiroshi Onishi2, and Utaroh Motosugi2
1MR Collaboration and Development, GE Healthcare, Hino, Japan, 2Radiology, University of Yamanashi, Chuo, Japan, 3MR Collaboration and Developement, GE Healthcare, Madison, WI, United States, 4MR Engineering, GE Healthcare, Waukesha, WI, United States
Synopsis
We demonstrated the feasibility of breath hold-free dynamic MRI of the liver using stack-of-stars acquisition with super high temporal frame rate (0.5s/phase) reconstruction. Stack-of-stars acquisition with soft gating technique enabled to acquire sufficient quality of dynamic MRI without breath-holdings. The super high frame rate reconstruction provided the better time-intensity curves, which enabled to capture accurate time-to-peak enhancement of each vessel, a second bolus pass in the aorta, and the peak delay from splenic vein to main portal vein. This technique is feasible for the comprehensive understandings of hemodynamics in arterial and portal venous circulation and abdominal organs.
Introduction
In examinations of abdominal dynamic MRI, we often failed to obtain sufficient image quality due to limited SNR and breath hold failure of the patients. The continuous stack-of-stars acquisition with retrospective respiratory motion suppression is expected to enable breath hold-free dynamic MRI. Another advantage of stack-of-stars acquisition is extremely high temporal frame rate while keeping sufficient SNR. Super high temporal frame rate, e.g. <1 second per frame, may breed new idea in diagnostic strategy and functional assessment of abdominal MRI. In this study, we revealed the feasibility and utility of super high temporal frame rate reconstruction by analyzing the time-intensity curves.Methods
In this study, we used recently developed LAVA-Star pulse sequence, a stack-of-stars acquisition with golden angle and intermittent fat suppression pulse1-3. Dynamic LAVA-Star acquisition was performed in 4 subjects under free-breathing condition with the imaging parameters shown in Fig.1. The contrast agent (gadoteridol, 0.2mL/kg body weight) was injected at the rate of 2.0 ml/s followed by 20ml saline flush. Total of 1000 radial spokes were acquired in ~2 minutes continuously. For typical frame rate reconstruction, 10 phases with 200 spokes per phase were reconstructed using 100 spokes offset between phases, which was equivalent to 12.6 s/phase. For high frame rate reconstruction, 226 phases were reconstructed with 4 spokes offset between phases, which was equivalent to 0.5 s/phase. In each phase reconstruction, ARC algorithm was used before Fourier transformation in kz direction and CG-SENSE algorithm was used for in-plane reconstruction4. The soft-gating, a retrospective gating technique, was used to suppress the image blur due to respiratory motion5. The time-intensity curves of aorta, portal vein and liver parenchyma from the two reconstructions were compared.Results
Fig.2 shows the images of dynamic LAVA-Star acquisition with typical (10 phases, 12.6 s/phase) and super high (226 phases, 0.5 s/phase) temporal frame rate reconstruction. Fig.3 shows the time-intensity curves of aorta, portal vein and liver parenchyma in the typical and high frame rate in the four cases. In case #1, #2 and #3, the second pass of the contrast agent in the aorta (relatively higher enhancement in the aorta due to a contrast bolus coming back to the heart via inferior vena cava) could be identified only in the curve of high frame rate reconstruction (Fig.3, arrow). In case #4, the peak enhancement in the aorta could be clearly seen only in the high frame rate reconstruction (Fig.3, arrow head). In all cases, signals of the aorta raised in biphasic manner in the high frame rate reconstruction. The time-to-peak enhancements of aorta, main portal vein and liver parenchyma, mesenteric circulation time (the time from aorta peak to main portal vein peak) were summarized in Fig.4. Fig. 5 shows other ideas to use super high temporal frame rate in the analysis of hemodynamic of the vessels. Since the portal flow curve would be the composite of two flow curves (splenic and superior mesenteric vein [SMV]), the difference between the curves of splenic vein and portal vein should be due to mesenteric venous flow.Discussion
The super high temporal frame rate reconstruction is feasible using stack-of-stars acquisition for dynamic MRI. It could show the better conspicuity of the aorta peak enhancement of the first and second passes and enable to measure mesenteric circulation time, which was consistent with theoretical value. Analyses of the difference in time-to-peak enhancement or peak contrast value may improve the clinical value of dynamic MRI. These observations would provide the better understandings of the arterial and portal venous circulation system. Another notable observation in the high frame rate reconstruction was that the rise of the aorta signal showed biphasic uptake, which is not observed in the conventional MR or CT dynamic scan. The reason of the biphasic behavior would be a transition of syringes from contrast agent to saline flush, i.e. the injection was briefly stopped during the injector switches the pushing syringes from the contrast agent to saline. Of course, high temporal frame rate is useful for capturing the precisely optimized arterial and portal venous phase by retrospectively analyzing the time-intensity curve.Conclusion
Stack-of-stars acquisition enables dynamic MRI under free-breathing. Super high temporal frame rate reconstruction improves the understandings of hemodynamics in arterial and portal venous circulation and abdominal organs.Acknowledgements
No acknowledgement found.References
- Peters DC, Korosec FR, Grist TM, et al. Undersampled projection reconstruction applied to MR angiography. Magn Reson Med 2000;43(1):91-101
- Chandarana H, Block TK, Rosenkrantz AB, et al. Free-Breathing Radial 3D Fat-Suppressed T1-Weighted Gradient Echo Sequence. Investigative Radiol 2011;46(10):648-653
- Zhang T, Cashen TA, Wang K, et al. Fast motion robust abdominal stack of stars imaging using coil compression and soft gating. In proceedings of the 25th Annual Meetings of ISMRM, Honolulu, HI, 2017. p.1284
- Pruessmann KP, Weiger M, Bornert P, et.al Advances in Sensitivity Encoding With Arbitrary k-Space Trajectories. Magn Reson Med 2001;46:638-651
- Johnson KM, Block WF, Reeder SB et.al. Improved least squares MR image reconstruction using estimates of k-Space data consistency. Magn Reson Med 2012;67(6):1600-1608
Figures
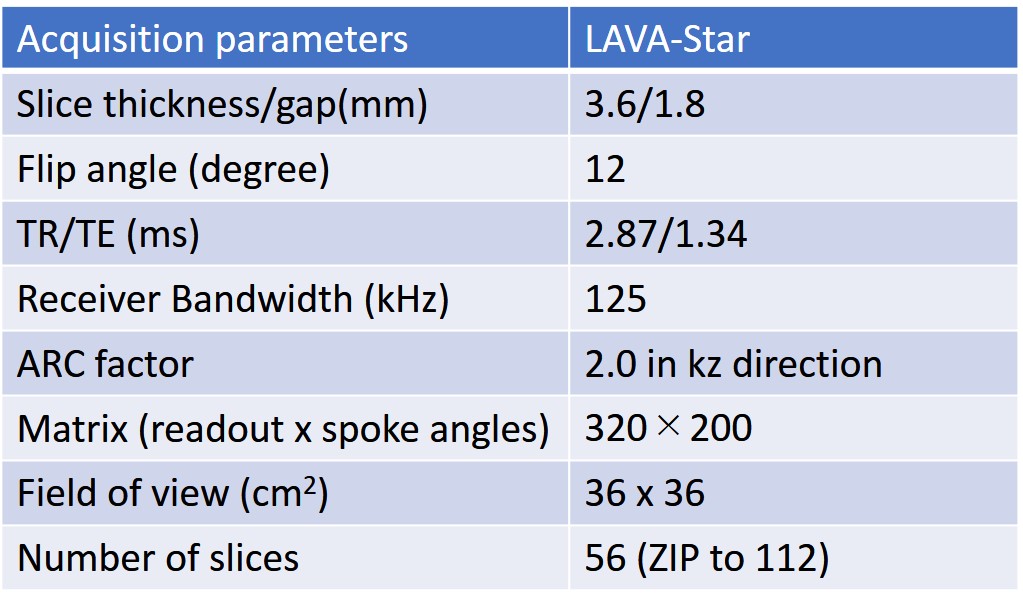
Fig.1: Scan parameters of LAVA Star used in this
study.
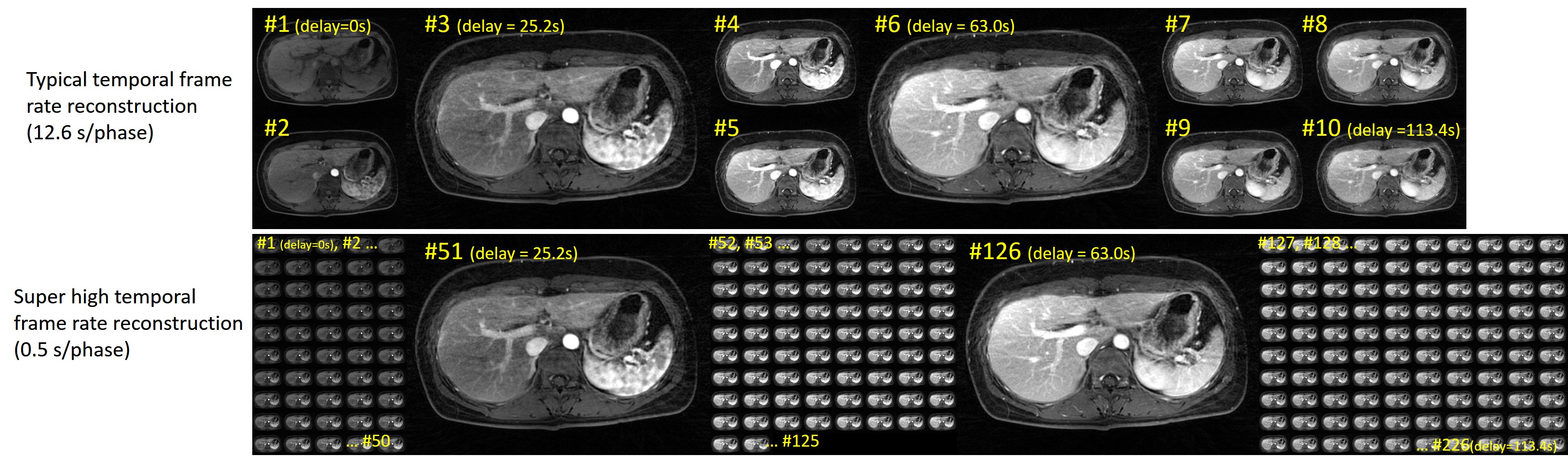
Fig.2 Representative images of dynamic LAVA Star
images with the typical frame rate reconstruction (10 phases, 12.6 s/phase: Top)
and super high temporal frame rate reconstruction (226 phases, 0.5 s/phase:
Bottom).
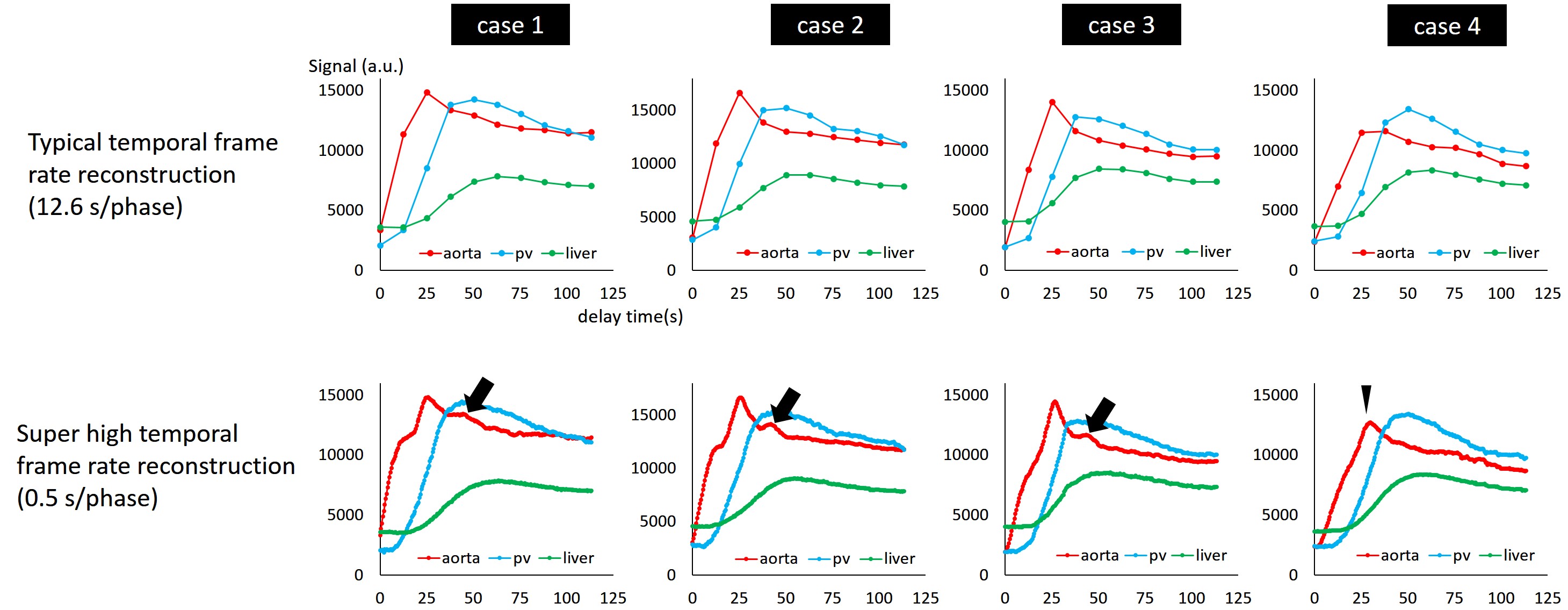
Fig.3 Time-intensity curves of aorta (red), main portal
vein (pv, blue) and liver parenchyma (green) obtained from the typical 12.6
s/phase frame rate (top) and the high 0.5 s/phase frame rate (bottom). In case #1, #2 and #3, the second bolus pass
in the aorta was observed only in the high frame rate reconstruction (arrows).
In case #4, the aorta peak (time-to-aortic peak) could be clearly seen in the
high frame rate (arrow head).
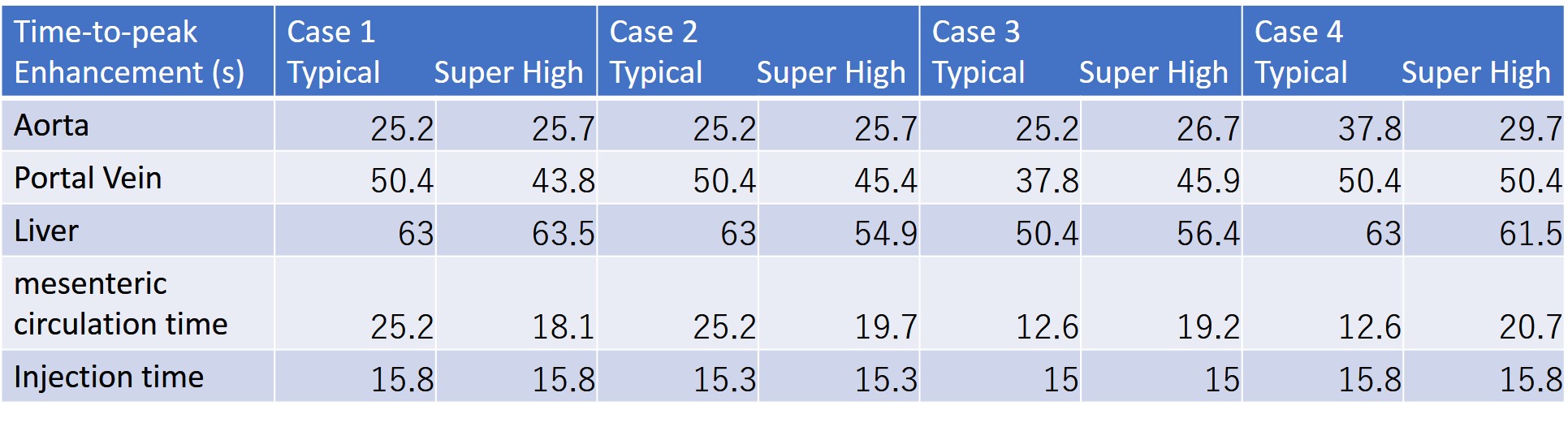
Fig.4: Time-to-peak enhancement in the aorta, main portal
vein and liver parenchyma, and mesenteric circulation time measured in the
typical and the super high frame rate reconstruction in addition to the
injection time. These times were less
varied in the super high frame rate reconstruction compared with typical frame
rate. Theoretically, time-to-peak enhancement and mesenteric circulation time
depend on the way of contrast injection, rather than patients-oriented factors.
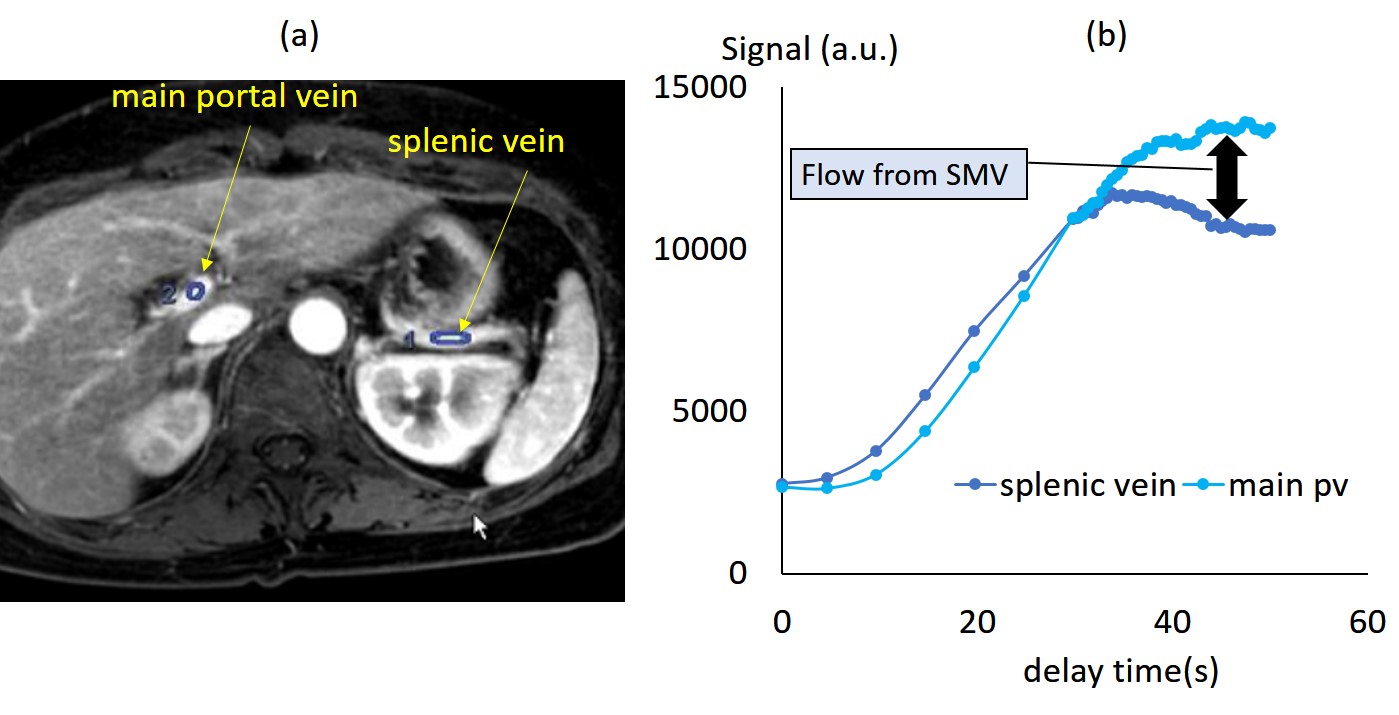
Fig. 5: (a and b) The time-intensity curves of splenic
vein and main portal vein could help understand the hemodynamics of the
headstreams (splenic and mesenteric venous flow) and portal flow. The splenic
venous flow decays after the peak, while enhancement continues in the portal
vein, suggesting mesenteric circulation takes longer time than splenic
circulation.