1779
Quantitative Assessment of Liver Function using Hepatocyte Fraction on Gd-EOB-DTPA-Enhanced MRI1the Third People’s Hospital of Nantong, Nantong, China, 2Philips Healthcare, Shanghai, China
Synopsis
The purpose of this study was to investigate the ability of hepatocyte fraction on Gd-EOB-DTPA-enhanced MRI for the assessment of liver function of HBV-induced cirrhosis. We used Look-Locker sequences to acquire T1 mapping images pre and post-contrast at 20 minutes after Gd-EOB-DTPA administration, hepatocyte fraction (HeF) and KHep values were measured. Our study showed that hepatocyte fraction is useful for the evaluation of liver function of HBV-induced cirrhosis.
INTRODUCTION
Assessment of the liver function is an essential procedure for preventing hepatic failure and for the medical management of patients with hepatic dysfunction. Gadoxetic acid (Gd-EOB-DTPA) is a hepatocyte-specific contrast agent for MRI of the liver, uptake and metabolism of Gd-EOB-DTPA is related to hepatocyte function1. The purpose of this study is to evaluate the ability of hepatocyte fraction using Gd-EOB-DTPA-enhanced MRI for the assessment of liver function of HBV-induced cirrhosis. Our study based on a simple pharmacokinetic model2( Fig.1) and the ΔR1 values to calculate.
R1(t) = 1 / T1(t) t: time after contrast injection (min)
ΔR1 = [ R1(t) - R1(0) ]
Hepatocyte fraction = ΔR1Hepatobilitary / (ΔR1Hepatobilitary+ΔR1BloodEES)
KHep = (ΔR1Hepatobilitary / ΔR1BloodEES) / t
PURPOSE
To assess the ability of hepatocyte fraction on Gd-EOB-DTPA-enhanced MRI for the evaluation of liver function.
METHODS
89 patients (64 Males, 25 Females; mean age 52±11 years) who underwent Gd-EOB-DTPA-enhanced MRI were classified in to 3 groups as follows: normal liver function (NLF), n=22; HBV-induced liver cirrhosis with Child-Pugh A (LCA), n=46; Child-Pugh B (LCB), n=21. Look-Locker sequences with exactly the same scan parameters and geometry position (the level of porta hepatis) were performed pre and post-contrast at 20 minutes after Gd-EOB-DTPA administration to acquire T1mapping. All the data were acquired on 3T MR System. Hepatocyte fraction (HeF) and KHep values were measured, four regions of interest (ROIs) were sparsely placed in both lobes of the liver. One-way ANOVA was used to compare HeF and KHep. ROC curve analysis was performed to compare the diagnostic performance of HeF and KHep in discriminating NLF group from LCA group and LCA group from LCB group.RESULTS
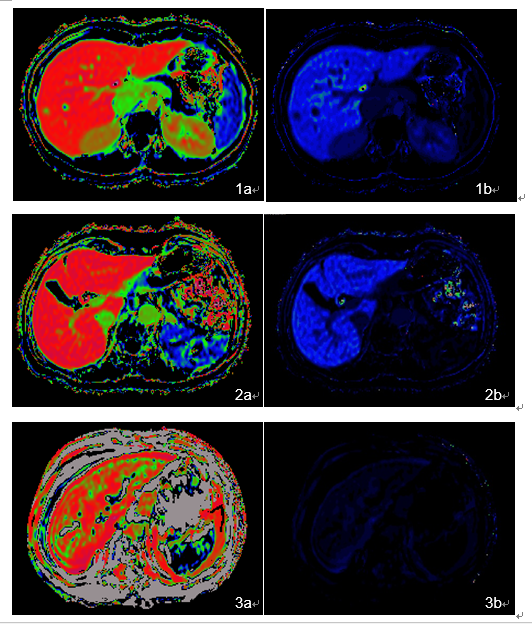
HeF and KHep values of different groups were shown in table 1 (Fig.2). HeF and KHep values progressively decreased from NLF, LCA to LCB group. HeF with LCB group was significantly different (P<0.05) in comparison with that of NLF group or LCA group, no significantly different (P>0.05) was found between NLF group and LCA group. KHep showed significant differences (P<0.05) among the three groups.
Diagnostic performance for discriminating NLF group from LCA group were shown in table 2.
Diagnostic performance for differentiating LCA group from LCB group were shown in table 3.
DISCUSSION
Gd-EOB-DTPA can be specifically taken up by hepatocytes and excreted through the biliary tract, the intracellular transport mechanisms of Gd-EOB-DTPA are mediated by organic anion-transporting polypeptide 1 (OATP1), the reduced Gd-EOB-DTPA uptake may be either due to a decreased number of normal hepatocytes in cirrhotic liver or due to decreased expression of OATP1 or diminished OATP1 activity on the surface of hepatocytes3-4. Hepatocyte fraction was not affected by blood and extracellular extravascular space (EES)2, it had two indices such as HeF and KHep, which reflected the ability of hepatocytes uptake and were relevant to OATP1. Previous study showed that hepatocyte fraction was useful for the staging of liver fibrosis5. In our study, HeF and KHep values showed a constant decrease from NLF, LCA to LCB group, HeF and KHep of LCB group were significantly different in comparison with those of NLF or LCA group. AUCs of HeF and KHep for discriminating NLF from LCA group were 0.607 and 0.800, AUCs of HeF and KHep for differentiating LCA from LCB group were 0.954 and 0.916.CONCLUSIONS
Hepatocyte fraction based on Gd-EOB-DTPA- enhanced T1 mapping MRI is an efficient diagnostic tool for the evaluation of Liver function.Acknowledgements
No acknowledgement found.References
1 Katsube T, Okada M, Kumano S, et al. Estimation of liver function using T1 mapping on Gd-EOB-DTPA-enhanced magnetic resonance imaging[J]. Invest Radiol, 2011, 46(4): 277-283.
2 ahlqvist Leinhard O, Dahlström N, Kihlberg J, et al. Quantifying differences in hepatic uptake of the liver specific contrast agents Gd-EOB-DTPA and Gd-BOPTA: a pilot study[J]. Eur Radiol, 2012, 22(3): 642-653.
3 Tsuda N, Harada K, Matsui O. Effect of change in transporter expression on gadolinium-ethoxybenzyl-diethylene triamine pentaacetic acid-enhanced magnetic resonance imaging during hepatocarcinogenesis in rats [J]. J Gastroenterol Hepatol, 2011, 26(3): 568-576.
4 Ba-Ssalamah A, Bastati N, Wibmer A, et al. Hepatic gadoxetic acid uptake as a measure of diffuse liver disease: Where are we? [J]. J Magn. Reson. Imaging, 2017, 45(3): 646-659.
5 Pan S, Wang XQ, Guo QY. Quantitative assessment of hepatic fibrosis in chronic hepatitis B and C: T1 mapping on Gd-EOB-DTPA-enhanced liver magnetic resonance imaging[J]. World J Gastroenterol. 2018, 24(18): 2024-2035.
Figures
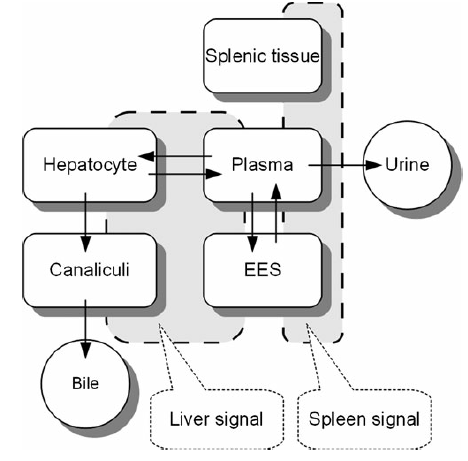

Table 1 HeF and KHep values of different groups.