1775
Clinical, technical, and biochemical predictors of adequate hepatobiliary phase enhancement on Gadobenate-Dimeglumine-enhanced MRI of the liver in patients with chronic liver disease and HCC1Department of Radiology, The third affiliated hospital of Sun Yat-sen University, guangzhou, China, 2Department of Radiology, University of California at San Diego, La Jolla, CA, United States
Synopsis
Liver dysfunction impairs the uptake of gadobenate dimeglumine by liver parenchyma, which reduces hepatocellular carcinoma (HCC) conspicuity on hepatobiliary phase (HBP) images. Although the effect of Child-Pugh class and some biologic factors have been investigated, there is a paucity of data on other plausible predictors of HBP adequacy. Here we show that elevated albumin level, prolonged HBP delay time, and absence of liver cirrhosis predict HBP adequacy on gadobenate-MRI in patients with chronic liver disease and HCC. In the subset of patients with cirrhosis and HCC, adequate HBP was associated with elevated serum creatinine level and prolonged HBP delay time.
Introduction
Gadobenate dimeglumine is a liver-specific contrast agent with dual properties of an extracellular agent and a hepatobiliary contrast agent1. Gradually taken up by functional hepatocytes and excreted into bile, this agent produces liver parenchyma enhancement in the hepatobiliary phase (HBP) 1 to 3 hours after administration2,3, which can help in the detection of hepatocellular carcinoma (HCC), as well as its differentiation from benign precursor lesions and vascular pseudolesions. Adequate liver enhancement on HBP is crucial for realizing these diagnostic benefits. However, liver dysfunction impairs the uptake of gadobenate by liver parenchyma, which reduces HCC conspicuity on HBP images4. Although a few studies showed that Child-Pugh class, renal function stage, and some serum liver chemistries may predict enhancement adequacy in the HBP4, 5, 6, there is paucity of data on other plausible predictors of HBP adequacy including HBP delay time and liver cirrhosis. The purpose of this study was to investigate the effect of HBP delay time, liver cirrhosis and other liver biologic factors on HBP adequacy on gadobenate-MRI in patients with chronic liver disease and histology-proven HCC.Methods
Our institutional review board approved this retrospective cohort study with waived informed consent requirement. From March 2016 to June 2018, 206 patients with chronic liver disease and histology-proven HCC and liver fibrosis stage underwent 1.5T or 3.0T gadobenate-MRI with acquisition of HBP images 1-3 hours after injection in our hospital. Blinded to clinical, laboratory, and pathologic information, two abdominal radiologists (6 and 25 years of liver MRI experience), reviewed the MR images independently, scored HBP adequacy, documented the number of HCC lesions, characterized the signal intensity of each HCC in the HBP. HBP adequacy was scored according to LI-RADS v20187 as adequate if the parenchyma was unequivocally hyperintense relative to hepatic blood vessels during the HBP and suboptimal otherwise. Discordances were resolved by consensus. After the above data were locked, the radiologists recorded the HBP delay time. Potential predictors for adequate HBP were analyzed using univariate and multivariate logistic regression. Variables with P˂0.05 in univariate logistic regression analysis were applied to a multivariate logistic regression analysis. The accuracy, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and the area under receiver operating characteristics curves (AUROC) of the multivariate models were estimated. Subgroup analysis was performed in patients with liver cirrhosis and HCC.Results
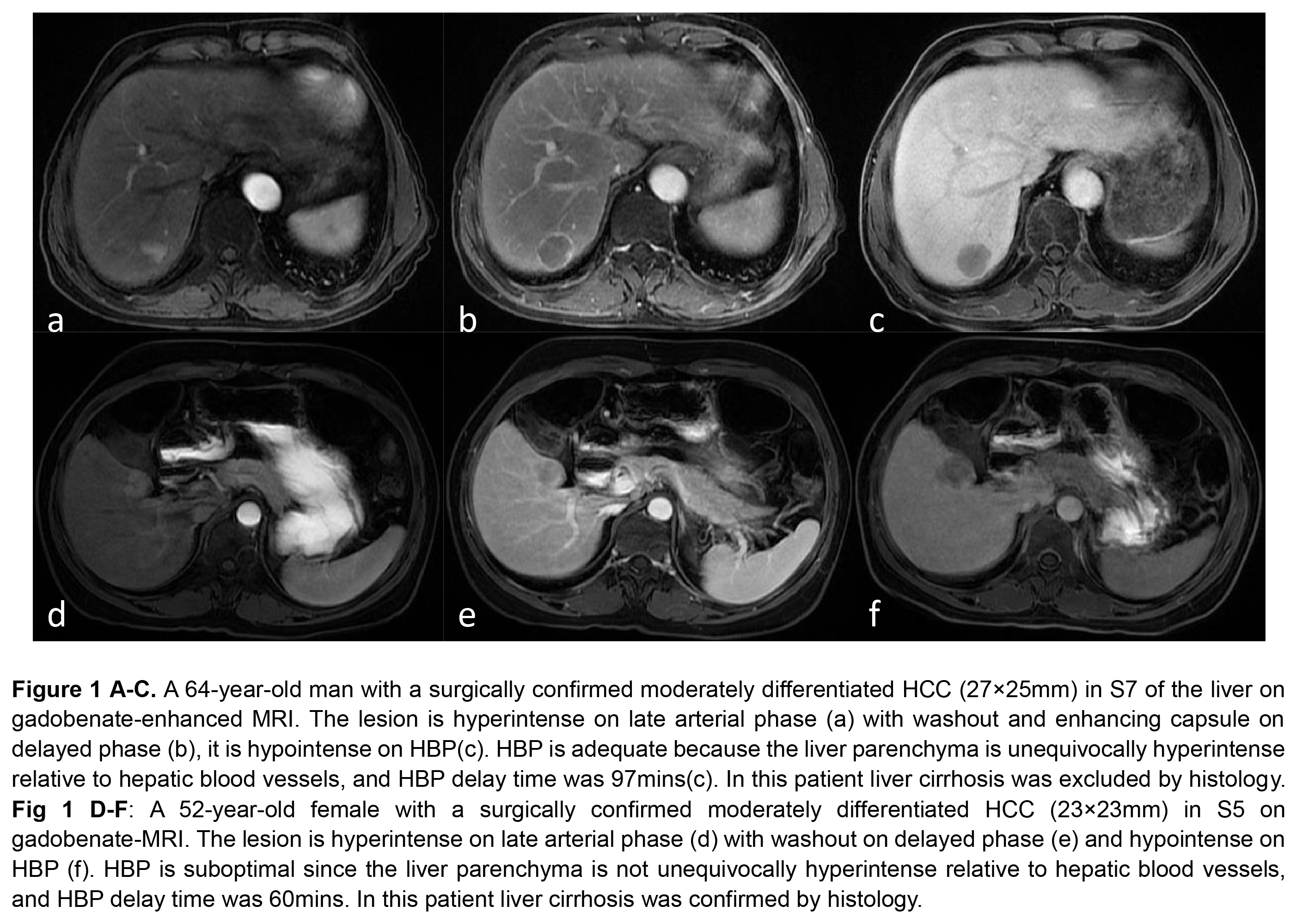
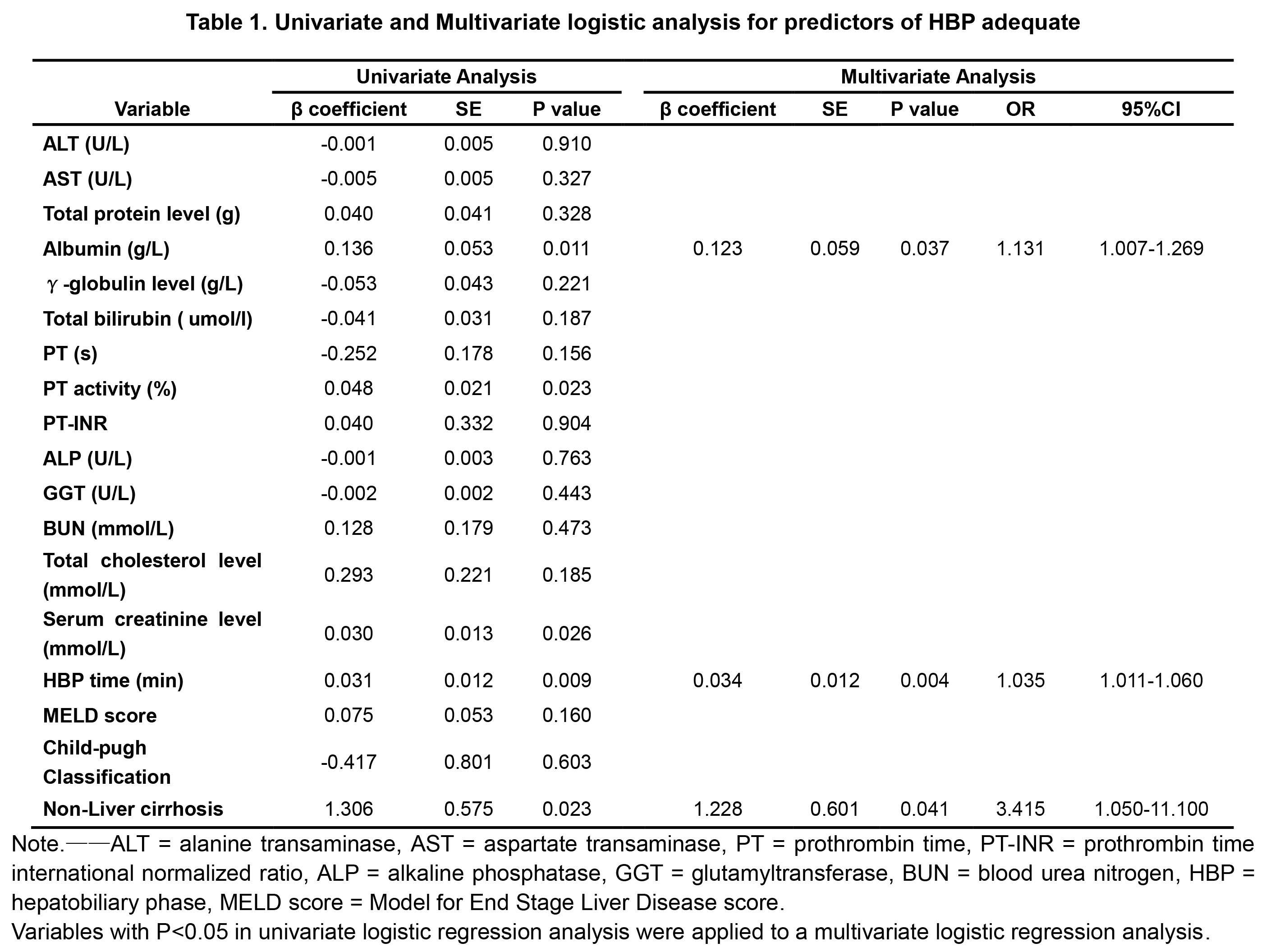
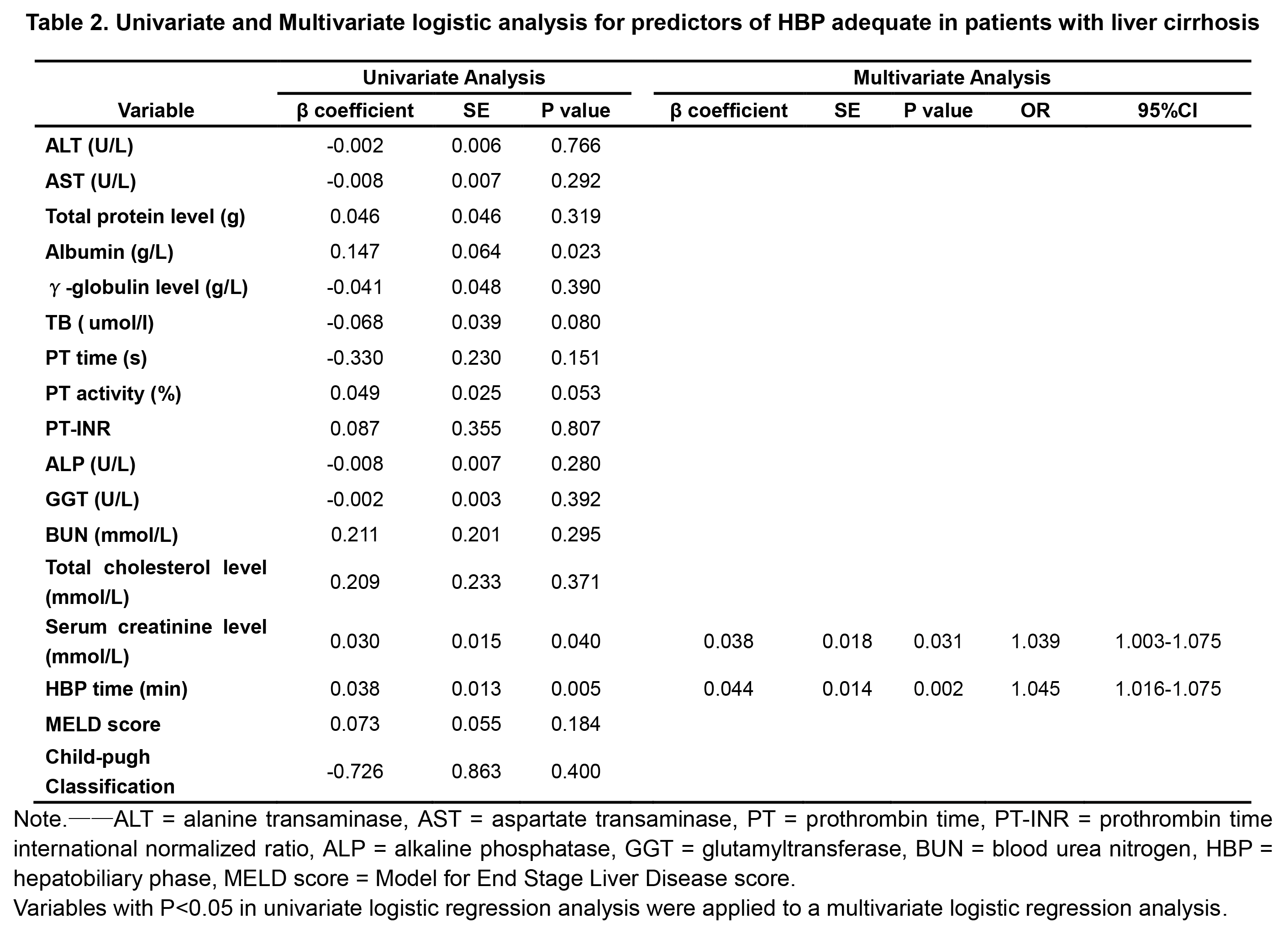
Liver cirrhosis was found in 116/206 (56.3%) patients. HBP was adequate in 185/206 (89.8%) patients overall. HBP was suboptimal in 17/116 (14.7%) patients with liver cirrhosis and in 4/90 (4.4%) patients without liver cirrhosis. In the 21 patients with suboptimal HBP, HCCs were hypointense in 18 (86%) and isointense in 3 (14%) (Figure 1). Albumin (OR=1.131, p=0.037), HBP delay time (OR=1.035, p=0.004), and absence of liver cirrhosis (OR=3.415, p=0.041) were significant, independent predictors of HBP adequacy (Table 1) overall. The accuracy, sensitivity, specificity, PPV, and NPV for predicting adequate HBP were 78.2%, 79.5%, 66.7%, 95.5% and 26.9%, respectively. The AUROC was 0.77. In the subgroup analysis, adequate HBP was associated with serum creatinine level (OR=1.039, p=0.031) and HBP time (OR=1.045, p=0.002) (Table 2). The accuracy, sensitivity, specificity, PPV, and NPV of the predict model were 75.0%, 74.8%, 76.5%, 91.4%, and 65.0%, respectively. The AUROC was 0.80.Discussion
Our study demonstrated that the combination of serum albumin, HBP delay time, and absence of liver cirrhosis predicts HBP adequacy on gadobenate-MRI with 78.2% accuracy, 79.5% sensitivity, and 66.7% specificity. In patients with cirrhosis, serum creatinine level and HBP time were independent predictors of adequate HBP with 75.0% accuracy, 74.8% sensitivity, and 76.5% specificity. Further research is needed to assess the impact of HBP adequacy and of prolonging the HBP delay on diagnostic accuracy. Limitations of this study were its single-center, retrospective design and its focus on patients with chronic liver disease and histology-proven HCC, which may restrict generalizability.Conclusions
In a retrospective single-center study, elevated serum albumin level, prolonged HBP delay time, and absence of liver cirrhosis predicted HBP adequacy on gadobenate-MRI in patients with chronic liver disease and HCC. In patients with cirrhosis, elevated serum creatinine level and prolonged HBP time predicted HBP adequacy.Acknowledgements
The authors state that this study has received funding by National Natural Science Foundation of China grant 81271562 (JW) and Science and Technology Program of Guangzhou, China 201704020016 (JW).References
1. Scali EP, Walshe T, Tiwari HA, et al. A Pictorial Review of Hepatobiliary Magnetic Resonance Imaging With Hepatocyte-Specific Contrast Agents: Uses, Findings, and Pitfalls of Gadoxetate Disodium and Gadobenate Dimeglumine. Can Assoc Radiol J. 2017 Aug;68(3):293-307.
2. Manfredi R, Maresca G, Baron RL, et al. Gadobenate dimeglumine (BOPTA) enhanced MR imaging: patterns of enhancement in normal liver and cirrhosis. J Magn Reson Imaging. 1998 Jul-Aug;8(4):862-7.
3. Jeong WK, Byun JH, Lee SS, et al. Gadobenate dimeglumine-enhanced liver MR imaging in cirrhotic patients: quantitative and qualitative comparison of 1-hour and 3-hour delayed images. J Magn Reson Imaging. 2011 Apr;33(4):889-97.
4. Kim JY, Lee SS, Byun JH, et al. Biologic factors affecting HCC conspicuity in hepatobiliary phase imaging with liver-specific contrast agents. AJR Am J Roentgenol. 2013 Aug;201(2):322-31.
5. Zhao X, Huang M, Zhu Q, et al. The relationship between liver function and liver parenchymal contrast enhancement on Gd-BOPTA-enhanced MR imaging in the hepatocyte phase. Magn Reson Imaging. 2015 Jul;33(6):768-73.
6. Jingbiao Chen, Qungang Shan, Yao Zhang, et al. Impact of clinical and biochemical factors on adequacy of hepatobiliary (HPB) phase enhancement on Gadobenate-Dimeglumine-enhanced MRI of the liver. SCBT-MR, Washington DC, USA, 6-10 October 2018, Traditional poster.
7. American College of Radiology. Liver imaging reporting and data system version 2018. http://www.acr.org/quality-safety/resources/LIRADS.
Figures