1774
Preoperative Remnant Liver Function Evaluated by a Clinical-Available Gd-EOB-DTPA-Enhanced MR Imaging Protocol: Independently Significant Indicator in Predicting Posthepatectomy Liver Failure in HCC Patients1Center for Biomedical Imaging Research, School of Medicine, Tsinghua University, Beijing, China, 2Department of Radiology, Southwest Hospital, Third Military Medical University, Chongqing, China, 3Beijing Tsinghua Changgung Hospital, School of Medicine, Tsinghua University, Beijing, China
Synopsis
Preoperative remnant liver function evaluation is important for surgery planning and reducing posthepatectomy liver failure (PHLF) rate in hepatocellular carcinoma (HCC) patients. This study demonstrated that the remnant liver functions preoperatively evaluated by a clinical available Gd-EOB-DTPA-enhanced imaging protocol were the independently significant indicator in predicting PHLF after adjusting for other PHLF risk factors including sex, age, hepatitis, cirrhosis, preoperative blood serum indices, operation time, intraoperative blood loss and intraoperative blood transfusion in the multivariate logistic regression.
Introduction
Preoperative remnant liver function evaluation is important for surgery planning and reducing posthepatectomy liver failure (PHLF) rate in hepatocellular carcinoma (HCC) patients 1. In the previous study, we have demonstrated that the remnant liver functions preoperatively evaluated by a clinical available Gd-EOB-DTPA-enhanced imaging protocol were better than liver volume and ICG based liver function parameters in PHLF prediction 2. However, various risk factors such as patient related factors (hepatitis, cirrhosis, preoperative bilirubin level) and surgery related factors (intraoperative blood loss and transfusion, operation time) are associated with PHLF 3. Thus, in this study, the ability of the remnant liver function calculated by EOB-enhanced MR imaging in predicting PHLF was accessed using multivariate logistic regression considering other PHLF risk factors.Methods
This retrospective study was approved by the institutional review board, and the requirement for informed consent was waived. 205 HCC patients who underwent liver resection between 2015 and 2017 were recruited. The EOB-enhance MRI scan protocols and the post-processing procedure were the same as previous 2. Overall, the remnant liver functions (RFUR (ml/min), RFRE10 (ml)) based on a clinical-available EOB-enhance MRI were calculated by sum of these liver function parameters (uptake rate (UR), relative enhancement in 10 min (RE10)) of each pixel in the remnant liver regions. The indocyanine green (ICG) retention rate at 15 min (ICG R15) before liver resection and the remnant liver function based on ICG R15 (RFICG-K) were also accessed as previous 2. Blood serum examinations were performed before surgery and on or after postoperative day 5. Intraoperative parameters including operation time, blood loss and blood transfusion were recorded. The PHLF definition was according to the International Study Group of Liver Surgery (ISGLS) 4.
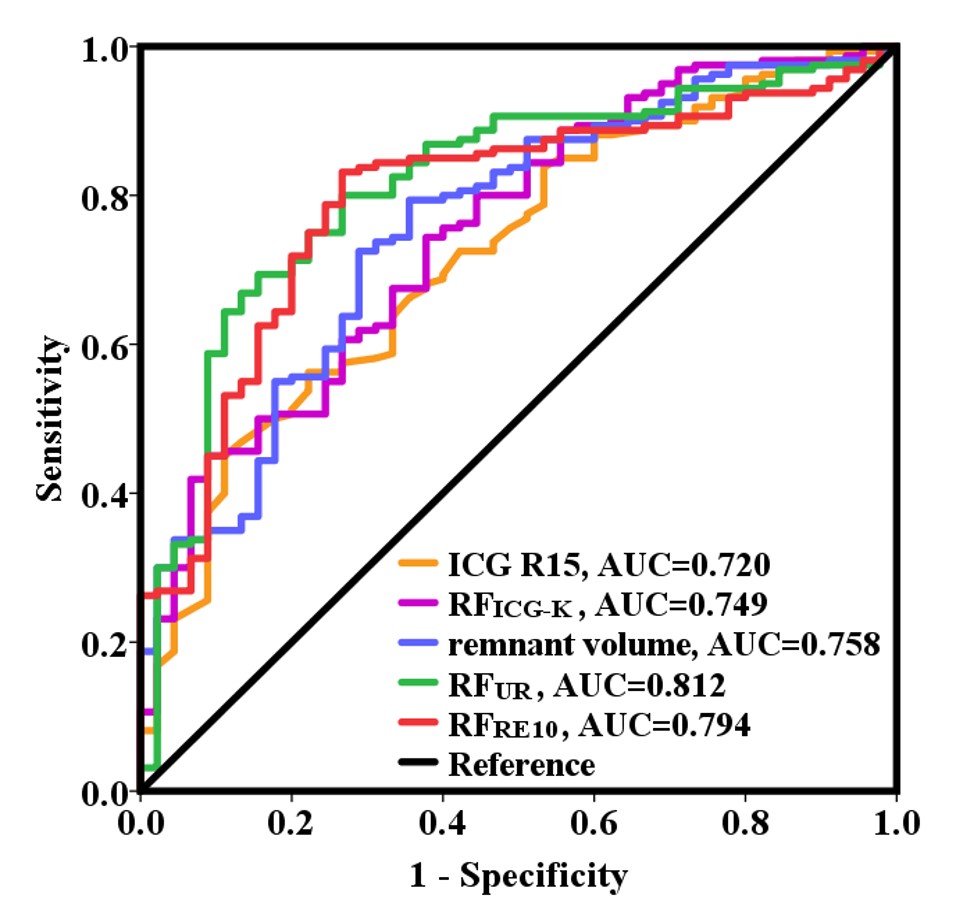
For patients with and without PHLF, the categorical variables were compared using Chi-square test and the continuous variables were compared using the two-tailed independent Student’s t test or Mann–Whitney U test. Univariate and multivariate logistic regression were performed to test the association between preoperative liver function parameters and PHLF. Receiver operating characteristics (ROC) analysis was applied to test the performance of preoperative liver function parameters to predict PHLF. The area under the ROC curves (AUC) were calculated.
Results
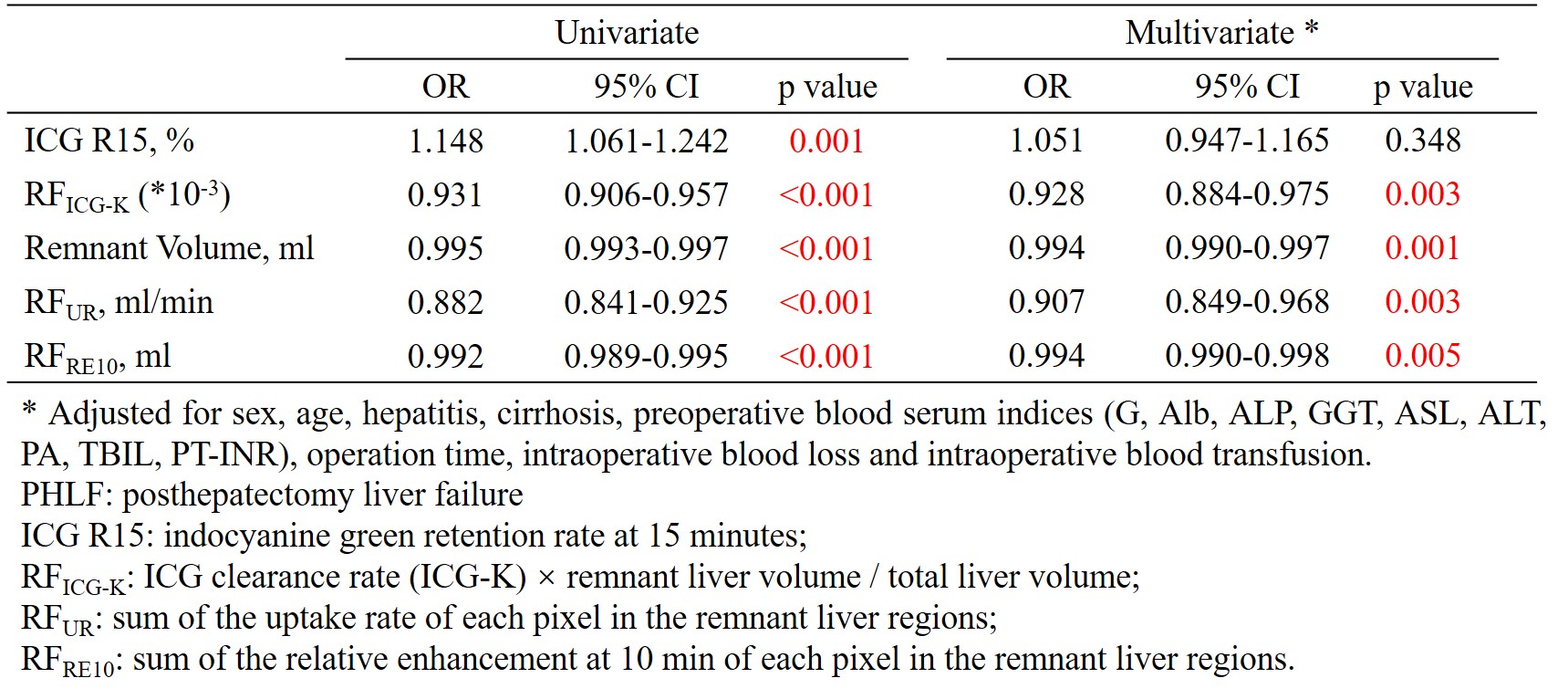
Characteristics of the patients were summarized in Table 1. 45 out of the 205 patients were found to have PHLF. Patients with PHLF showed significantly higher age, GGT, ASL, TBIL, PT-INR, operation time, intraoperative blood loss, intraoperative blood transfusion and lower Alb, PA than patients without PHLF (Table 1). Fig 1 showed the example preoperative UR and RE10 maps of one patient without PHLF (male, age 43) and one with PHLF (male, age 56). The remnant liver volume of the two patients were similar (840.2 ml vs. 837.0 ml). However, the patient with PHLF showed much lower RFUR and RFRE10 than the patient without PHLF (13.0 ml/min vs. 34.8 ml/min for RFUR, 253.4 ml vs. 637.2 ml for RFRE10). Overall, for preoperative liver function parameters, the patients with PHLF showed significantly lower preoperative RFICG-K, remnant volume, RFUR, RFRE10 and higher ICG R15 than patients without PHLF (Table 1, p < 0.001 for all the parameters). Significant association between preoperative liver function parameters and PHLF were found during univariate analysis (Table 2, p = 0.001 for ICG R15, p < 0.001 for others). After adjusting for other PHLF risk factors including sex, age, hepatitis, cirrhosis, preoperative blood serum indices (G, Alb, ALP, GGT, ASL, ALT, PA, TBIL, PT-INR), operation time, intraoperative blood loss and intraoperative blood transfusion, significant association between RFICG-K, the remnant liver volume, RFUR, RFRE10 and PHLF remained (Table 2, p = 0.003 for RFICG-K, p = 0.001 for the remnant volume, p = 0.003 for RFUR, p = 0.005 for RFRE10). Imaging remnant liver function parameters (RFUR and RFRE10) had larger AUC (0.812 and 0.794) than the remnant volume (0.758) and ICG based liver function parameters (ICG R15: 0.720 and RFICG-K: 0.749) (Fig 2).Discussion and Conclusion
The results of this study showed that the remnant liver function parameters evaluated by a clinical available Gd-EOB-DTPA-enhanced imaging protocol were the independently significant indicator in predicting PHLF after adjusting for other PHLF risk factors including sex, age, hepatitis, cirrhosis, preoperative blood serum indices, operation time, intraoperative blood loss and intraoperative blood transfusion in the multivariate logistic regression and had the larger AUC in the ROC analysis. Compare to RFRE10, RFUR needs much shorter scan time (5 min). Thus, RFUR may be the most suitable parameter for PHLF prediction considering its cost and performance in clinical practice.Acknowledgements
No acknowledgement found.References
1. Seyama Y, Kokudo N. Assessment of liver function for safe hepatic resection. Hepatol Res. 2009;39(2):107-16.
2. Yajie Wang, Lin Zhang, Jia Ning, Xinjing Zhang, Xuedong Wang, Shizhong Yang, Jiahong Dong, Huijun Chen. Preoperative Remnant Liver Function Evaluation using a Clinical-Available Gd-EOB-DTPA-Enhanced MR Imaging Protocol in HCC Patients. Proc Intl Soc Mag Reson Med 26. 2018.
3. Kauffmann R, Fong Y. Post-hepatectomy liver failure. Hepatobiliary Surgery and Nutrition. 2014;3(5):238-46.
4. Rahbari NN, Garden OJ, Padbury R, Brooke-Smith M, Crawford M, Adam R, et al. Posthepatectomy liver failure: a definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery. 2011;149(5):713-24.
Figures
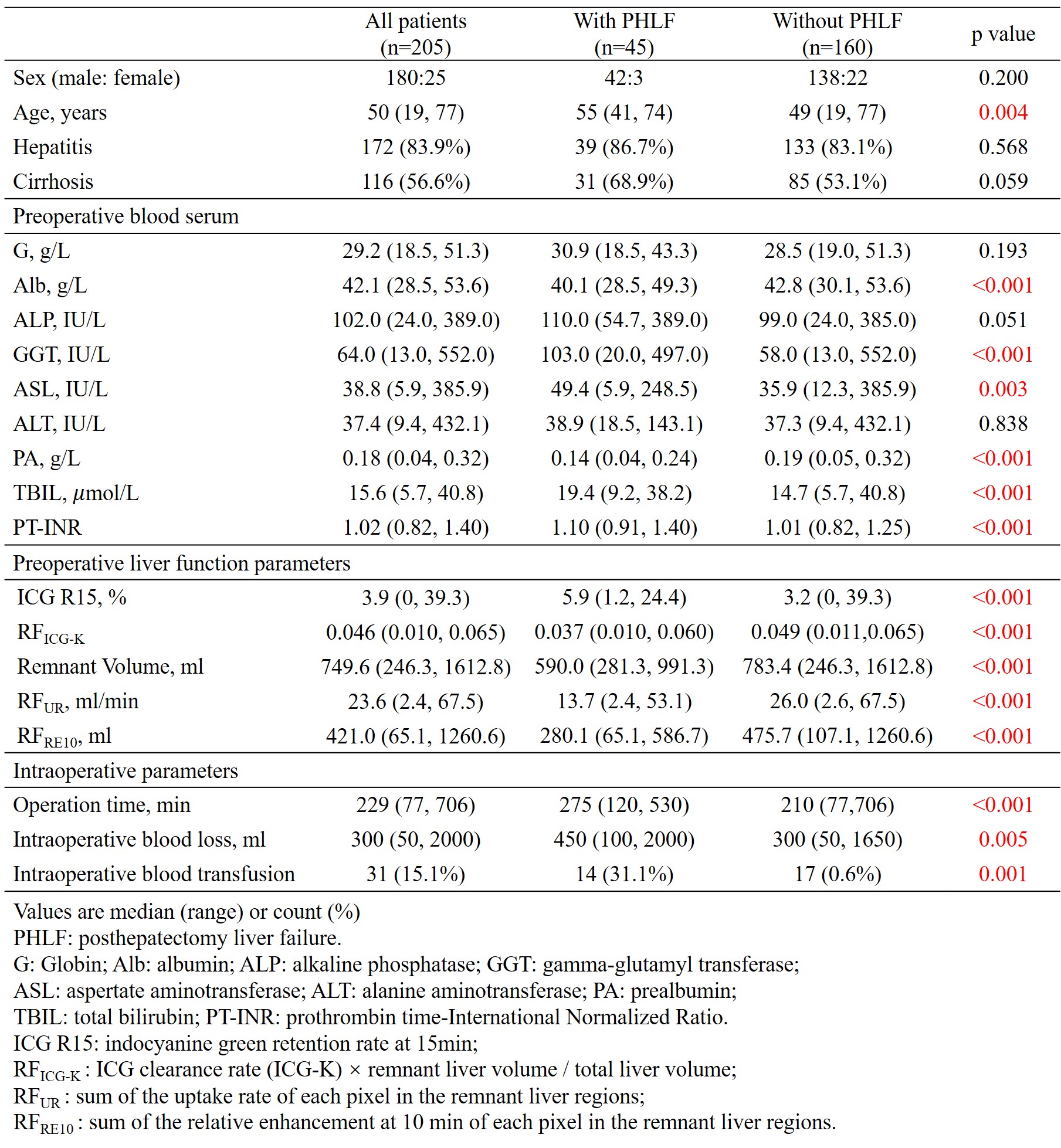
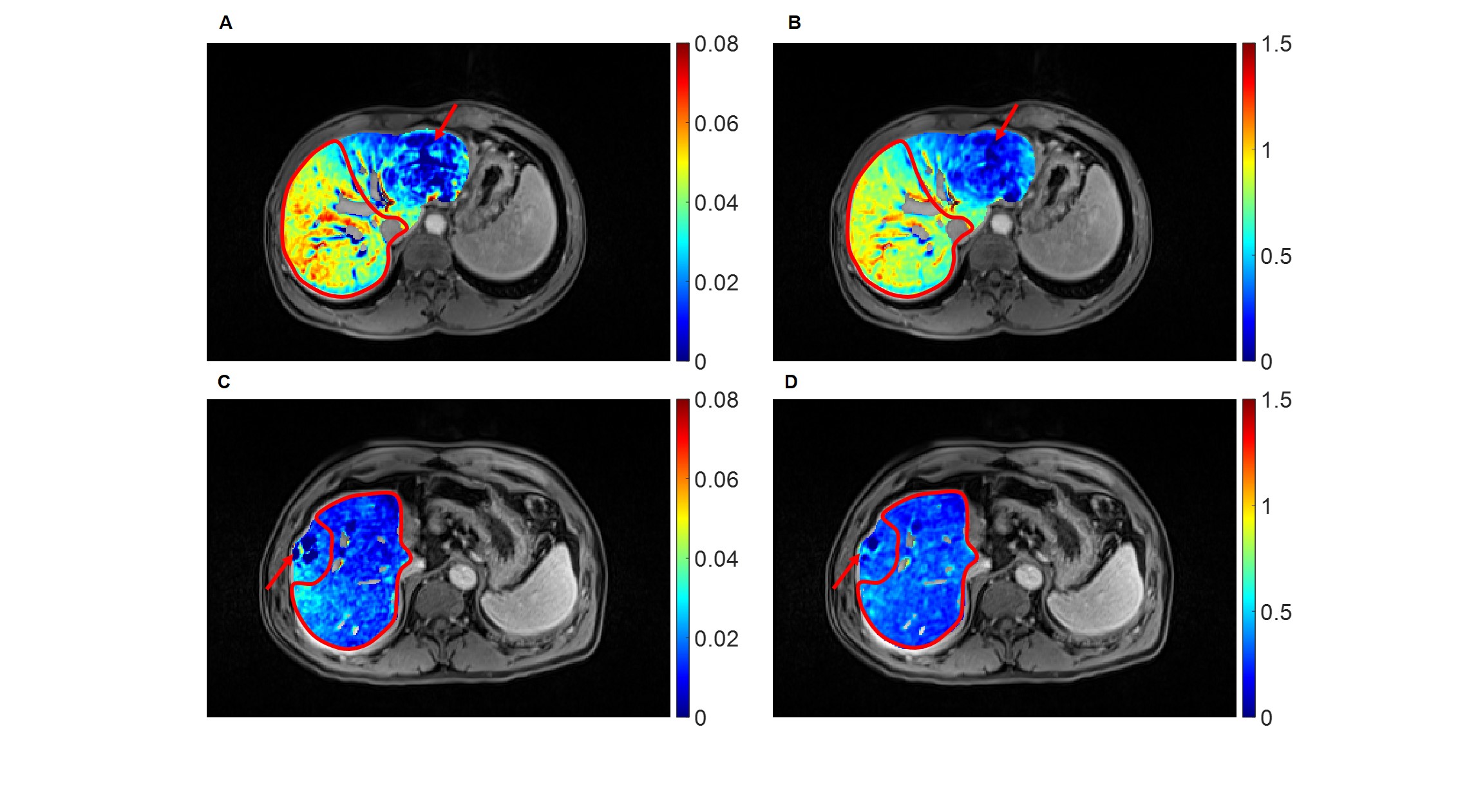
Fig 1. Uptake rate (UR) map (A) , relative enhancement at 10 min (RE10) map (B) of one patient (male, age 43) with HCC (arrow) who did not develop posthepatectomy liver failure. The remnant liver volume=837.0 ml, the RFUR=34.8 ml/min, the RFRE10=637.2 ml.
Uptake rate (UR) map (C) , relative enhancement at 10 min (RE10) map (D) of one patient (male, age 56) with HCC (arrow) who developed posthepatectomy liver failure. The remnant liver volume=840.2 ml, the RFUR=13.0 ml/min, the RFRE10=253.4 ml.
The remnant liver regions were outlined by the red contours.