1772
3D Stack-of-Stars Radial Imaging for Motion-Robust Free-Breathing Hepatobiliary Phase Imaging1Departments of Radiology, University of Wisconsin, Madison, WI, United States, 2Global MR Applications and Workflow, GE Healthcare, Madison, WI, United States, 3Global MR Applications and Workflow, GE Healthcare, Waukesha, WI, United States, 4Global MR Applications and Workflow, GE Healthcare, Houston, TX, United States, 5Biomedical Engineering, University of Wisconsin, Madison, WI, United States, 6Medical Physics, University of Wisconsin, Madison, WI, United States, 7Medicine and Emergency Medicine, University of Wisconsin, Madison, WI, United States
Synopsis
Free-breathing hepatobiliary phase imaging with gadoxetate disodium is challenging due to respiratory motion. This study examines an intrinsically motion-robust fat-suppressed T1-weighted 3D stack-of-stars gradient echo technique (LAVA Star) with soft gating. An estimate of respiratory motion is derived either from a navigator tracker with a wide acceptance window, which produces the best image quality, or self-navigation, which offers the most convenient workflow, particularly in challenging clinical situations. In either case, the retrospective soft gating reduces scan time variability compared to a conventional prospective navigator.
Introduction
Gadoxetate disodium (Eovist/Primovist, Bayer Healthcare, Berlin, Germany) is a liver-specific gadolinium-based MR contrast agent useful for characterization of focal liver lesions. The hepatobiliary phase is typically acquired 15-20 minutes after contrast. Very high resolution T1 weighted imaging can be performed using a free-breathing technique, such as LAVA (Liver Acquisition with Volume Acceleration) with a navigator tracker placed across the diaphragm. High spatial resolution free-breathing acquisitions can be performed during this phase because contrast has reached a quasi-steady-state and rapid breath-hold acquisitions are not necessary. 1
Robustness to motion artifacts remains a challenge for free-breathing techniques, particularly in patients with irregular respiratory patterns.2 The purpose of this study is to evaluate an intrinsically motion-robust 3D stack-of-stars (SoS) technique3 with three paradigms for motion compensation for motion-robust free-breathing high resolution hepatobiliary phase imaging. Specifically, we will evaluate: 1) prospective navigator tracking with a narrow acceptance window, 2) navigator tracking with a wide acceptance window combined with “soft gating”4,5, and 3) self-navigation (without a navigator tracker) made possible by the SoS trajectory frequently sampling the center of k-space combined with soft gating.
Methods
Patients undergoing a clinical liver exam with gadoxetate disodium on a 3T clinical MR system (MR750 or MR750w, GE Healthcare, Waukesha, WI, USA) were asked to provide written informed consent for an add-on IRB-approved research protocol.
For pseudorandomization, on even days of the month before the clinical hepatobiliary phase scan (LAVA with navigator tracker)1 beginning at 15 to 20 minutes post contrast, images were acquired in the axial plane using a fat-suppressed T1-weighted 3D SoS gradient echo technique (LAVA Star) with navigator tracker with the following parameters: flip angle: 35°, TR/TE/TI: 6.5/2.3/7.0 ms, receive bandwidth: ±62.5 kHz, FOV: 36.0 ´ 36.0 cm, slice thickness: 1.8 cm, frequency encodings: 320, radial lines set to match the estimated clinical scan time: 156, slices: 124, slice partial Fourier factor: 0.70, slice ARC acceleration factor: 1.5, navigator tracker acceptance window: 2.0 mm, estimated scan time: 4:59. After the clinical scan, the LAVA Star scan was repeated except with the following changes: navigator tracker acceptance window: 50.0 mm, radial lines set to match the estimated clinical scan time: 506. Respectively, on odd days of the month the order of research scans was switched. The actual scan times for the clinical and two research scans were recorded.
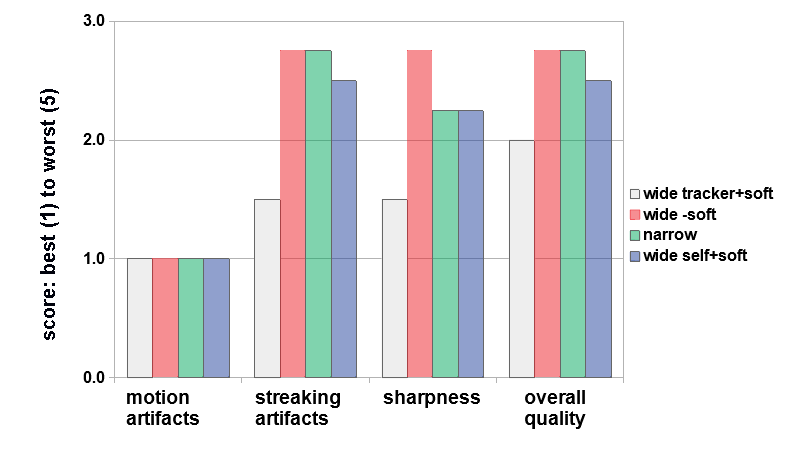
For the LAVA Star scan with the wide acceptance window, three reconstructions were performed: one with the navigator tracker signal as input to the soft gating algorithm, one with a self-navigation signal as input, and one without soft gating. All four research reconstructions were scored by a trained radiologist for motion and streaking artifacts on the following 5-point scale: none (1), minimal (2), moderate without diagnostic effect (3), severe but still diagnostically valuable (4), extensive and not diagnostic (5). Sharpness and overall quality were also scored on a scale from best (1) to worst (5).
Results
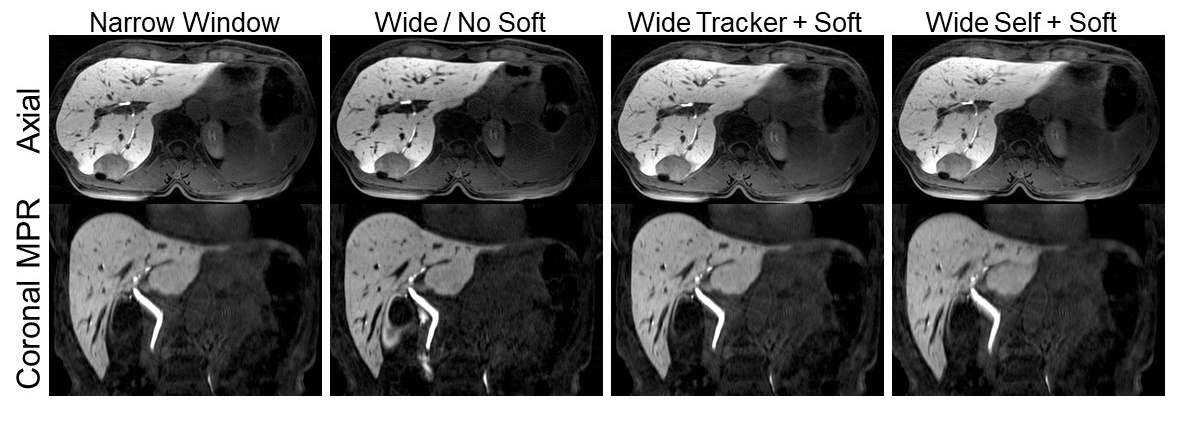
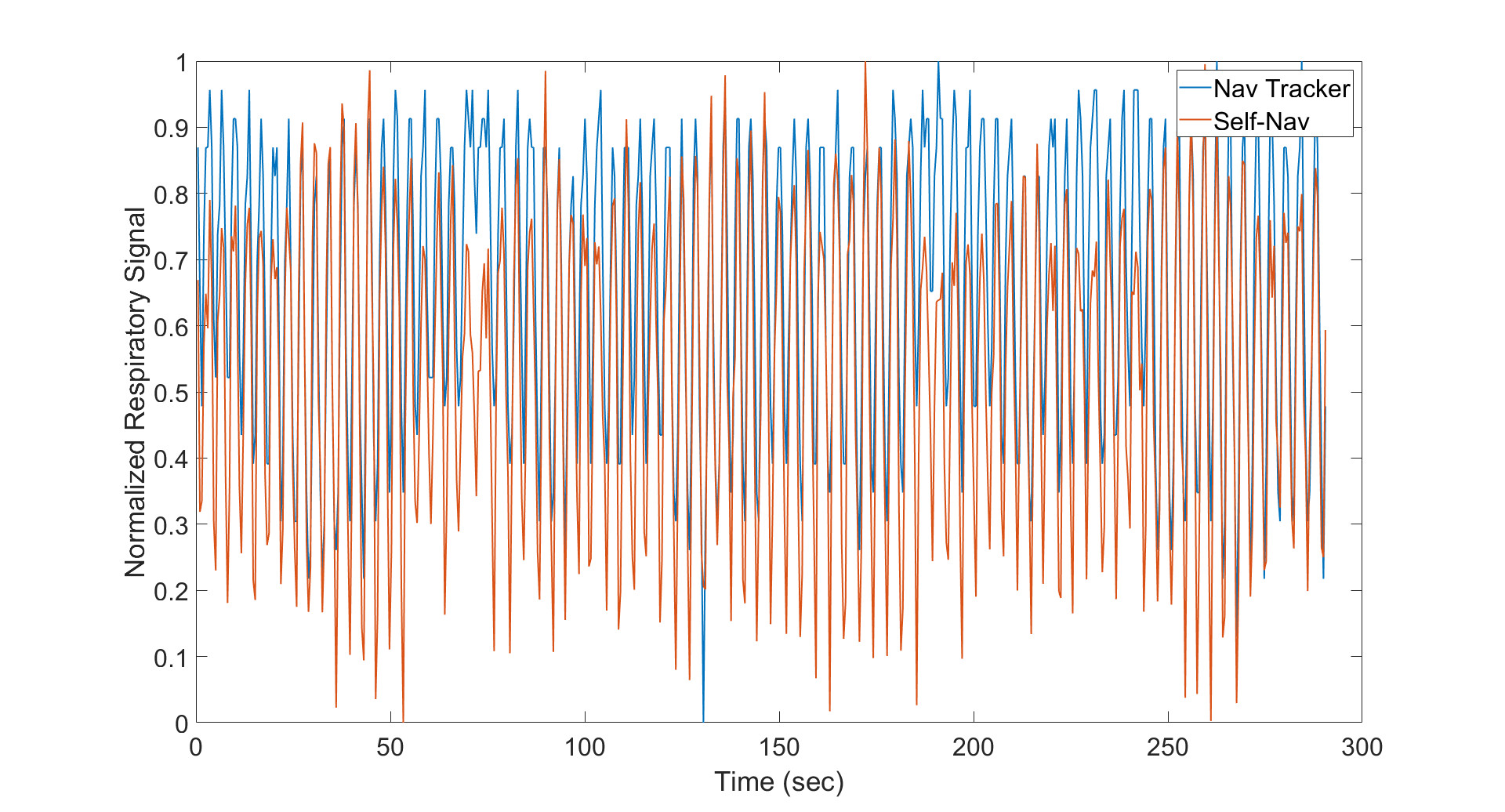
4 of 50 patients have been enrolled to date in this study. The mean ± standard deviation actual scan times for the clinical LAVA, research LAVA Star with narrow acceptance window, and research LAVA Star with wide acceptance window were 6:14 ± 1:06, 7:48 ± 2:51, and 5:59 ± 0:21, respectively. Figure 1 shows the results of scoring the four research reconstructions. Figure 2 displays an example case, and figure 3 an example overlay of the navigator tracker and self-navigation signals.Discussion
While the pulse sequence for the navigator tracker was unchanged between the clinical and research scans, the wide acceptance window resulted in shorter scan times with less variability. The difference in scan times between the clinical and research scans with the narrow acceptance window may be explained by the order of the scans since patients settle into a more regular respiratory pattern over time. While the trend shows that LAVA Star with the navigator tracker-based soft gating has the best scores on all metrics, self-navigation does provide a simpler workflow since there is no need to place the navigator tracker. Further, obtaining a dependable navigator tracker signal is challenging in certain patients, such as those with ascites, in which the edge of the diaphragm is obscured on imaging. Regardless, soft gating in general contributed to an improvement in image quality.Conclusion
LAVA Star with soft gating is a promising technique for motion-robust free-breathing hepatobiliary phase imaging with predictable scan times. Deriving an estimate of respiratory motion from a wide acceptance window navigator tracker improves image quality whereas self-navigation offers an option when the time and effort required to successfully place a navigator tracker is not worthwhile.Acknowledgements
No acknowledgement found.References
1. Nagle SK, Busse RF, Brau AC, Brittain JH, Frydrychowicz A, Iwadate Y, Reeder SB. High resolution navigated three-dimensional T₁-weighted hepatobiliary MRI using gadoxetic acid optimized for 1.5 Tesla. J Magn Reson Imaging. 2012;36:890-899.
2. McClellan TR, Motosugi U, Middleton MS, Allen BC, Jaffe TA, Miller CM, Reeder SB, Sirlin CB, Bashir MR. Intravenous Gadoxetate Disodium Administration Reduces Breath-holding Capacity in the Hepatic Arterial Phase: A Multi-Center Randomized Placebo-controlled Trial. Radiology. 2017;282:361-368.
3. Chandarana H, Block TK, Rosenkrantz AB, Lim RP, Kim D, Mossa DJ, Babb JS, Kiefer B, Lee VS. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Invest Radiol. 2011;46:648-653.
4. Johnson KM, Block WF, Reeder SB, Samsonov A. Improved least squares MR image reconstruction using estimates of k-space data consistency. Magn Reson Med. 2012;67:1600-1608.
5. Cheng JY, Zhang T, Ruangwattanapaisarn N, Alley MT, Uecker M, Pauly JM, Lustig M, Vasanawala SS. Free-breathing pediatric MRI with nonrigid motion correction and acceleration. J Magn Reson Imaging. 2015;42:407-420.
Figures