1770
Quantitative Measurement of Serial Contrast Agent Distribution between Liver and Blood in Patients with Chronic Liver Disease using T1 mapping1Department of Radiology and Imaging Sciences, Emory University, Atlanta, GA, United States
Synopsis
This study investigates the post-contrast time sensitivity of liver-to-blood partition coefficient. In vivo change in liver-to-blood contrast distribution was calculated at 3 time-points following contrast administration using a fast inversion-recovery Look-Locker T1 mapping approach. While measurement and exam time variation did not reveal a consistent equilibrium time threshold, results show that contrast distribution becomes increasingly different between chronic and non-chronic liver disease groups at least 5 minutes post-contrast, allowing possible measurement of liver extracellular volume fraction.
Introduction
Evaluation of extracellular volume fraction (ECV) has become widespread in cardiac MRI, serving as a surrogate for quantifying diffuse tissue fibrosis. This concept also has potential application in other areas, including liver fibrosis. A key requirement that governs the ECV relationship is the assumption of equilibrium extracellular contrast agent distribution between tissue compartments ([Gd]tissue ~ [Gd]plasma). This ensures the ratio of tissue-to-blood R1 change (ΔR1tissue/ΔR1blood) precisely represents the tissue partition coefficient1. While prior studies have determined this equilibrium to be as early as 3-5 mins post-contrast in cardiac applications2,3, no investigations have studied this time interval in liver. Therefore, the purpose of this preliminary study is to: 1) investigate the temporal change in contrast distribution (ΔR1tissue/ΔR1blood) in vivo, and 2) compare measured ΔR1tissue/ΔR1blood between chronic and non-chronic liver disease patient groups.Methods
Following IRB approval, serial T1 measurements were performed prospectively on 18 patients (8 female, avg age= 59.4 yrs) indicated for routine abdominal MRI. Even though no specific diagnostic inclusion or exclusion criteria was implemented, a retrospective survey of imaging findings found 8 patients with known chronic liver disease (CLD), and 10 patients without imaging evidence of CLD. Imaging was performed on a 1.5T Siemens Aera (Siemens Healthineers, Erlangen, Germany). T1 mapping was performed using an inversion-recovery (IR) single-shot spoiled gradient echo Look-Locker (IR-LL) approach, whereby multiple inversion time (TI) images were obtained following a single IR preparation4. Sampling of T1 recovery is dictated by the number of samples (#TI), sampling interval (ΔTI), and minimum, maximum sampling time (TImin, TImax). The following configuration employed for this study: #TI=32, ΔTI=170ms, TImin=100ms, and TImax=5700ms. Other imaging parameters were: FOV=380-425 x 300-340mm; matrix=192x154 (interpolated to 384x308); thickness=8mm; TR/TE=2.2/0.8ms; flip angle=8; bandwidth=1300Hz/px; GRAPPA=2; t=6s. One axial slice was positioned to include both right and left liver lobes. Following pre-contrast acquisitions, 0.1mmol/kg gadoteridol (Prohance, Bracco, Italy) was administered. Subsequent post-contrast T1 mapping was acquired with the following schedule: after portal-venous phase (t1 = +1.5-2.5mins), after delayed phase (t2 = +4-6mins), and after final diagnostic sequence (usually DWI, t3 = +8-12mins). Due to time restrictions of clinical exams, further time points were not acquired.
T1 maps were reconstructed inline by the system, accounting for the T1-shortening effects of steady-state spoiled gradient echo4. Mean and standard deviation (SD) were pooled from 3 regions-of-interest (ROI) in liver (2 right, 1 left lobe), avoiding major vessels, organ boundaries, and pathology. One ROI was recorded from descending aorta for blood T1. All ROIs were propagated to corresponding post-contrast T1 maps, whereby the ratio ΔR1 (for liver-to-blood) was calculated for each time point, including the propagation of T1 measurement error. The change in mean and standard deviation (SD) over time was statistically compared intra-individually, and between patient groups. Statistical significance was set to p<0.05.
Results
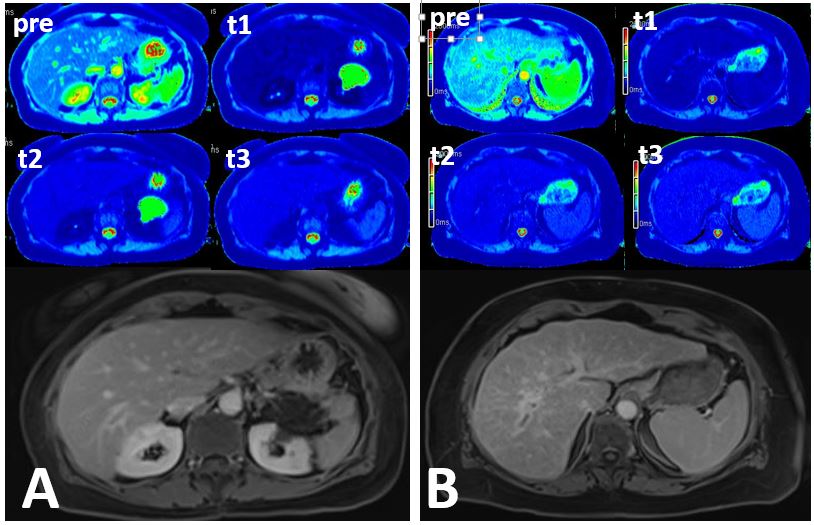
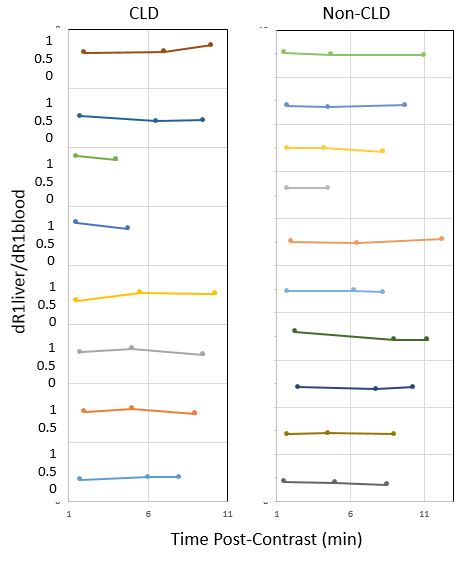
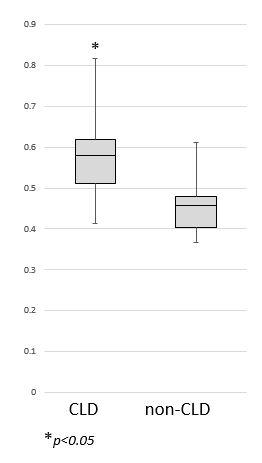
The average time points for post-contrast T1 mapping were t1=1.8min, t2=5.6min, and t3=9.5min post contrast. Three T1 maps were not obtained at the final time point (in 2 CLD and 1 non-CLD) due to patient cooperation issues, leaving n=15 for t3. The pooled mean and SD of pre-contrast liver and blood T1 was 555.1±39.6ms and 1525.3±56.3ms, respectively, while the average post-contrast T1 for liver and blood were: t1) 243.0±18.7ms and 200.8 ± 18.7ms; t2) 313.1±21.7ms and 309.5±20.3ms; and t3) 339.5±26.8ms and 359.6±22.8ms, respectively. Figure 1 shows an example of serial T1 maps in both a CLD and non-CLD case, and Figure 2 summarizes the change in ΔR1liver/ΔR1blood at each time interval for both CLD and non-CLD groups. From the cumulative data, no single time interval established a consistent equilibrium value that applied to all patients. From t2 to t3, 6/15 (40%) of patients showed significant change in ΔR1liver/ΔR1blood. However the non-CLD group exhibited more stability, with only 2/10 and 3/9 patients showing significant change between t1-t2 and t2-t3, respectively, compared to 4/8 and 3/6 in the CLD group. After grouping ΔR1liver/ΔR1blood according to time, data at t2 was found to show significant difference between CLD and non-CLD groups (p<0.5) (Figure 3).Discussion and Conclusion
While ΔR1liver/ΔR1blood remained stable for most cases between t2 (5.6min) and t3 (9.5min), allowing measurement of partition coefficient, a unique time interval was not universally measured in this patient group. Measurement error or tissue blood flow secondary to CLD are possible sources of variance. However, a significant difference in ΔR1liver/ΔR1blood was found between CLD and non-CLD groups following delayed-phased imaging, possibly allowing a mechanism for quantitative assessment of hepatic disease using ECV.Acknowledgements
No acknowledgement found.References
1. Wendland MF, Saeed M, Lauerma K, et al. Alterations in T1 of normal and reperfused infarcted myocardium after Gd-BOPTA versus Gd-DTPA on inversion recovery EPI. Magn Reson Med. 1997;37:448-56.
2. Jerosch-Herold, M., Sheridan, D.C., Kushner, J.D., et al. (2008). Cardiac magnetic resonance imaging of myocardial contrast uptake and blood flow in patients affected with idiopathic or familial dilated cardiomyopathy. AJP: Heart and Circulatory Physiology 2008;295:H1234–H1242
3. Sharma P, Socolow J, Patel S, Pettigrew RI, Oshinski JN. Effect of Gd-DTPA-BMA on blood and myocardial T1 at 1.5T and 3T in humans. J Magn Reson Imaging. 2006 Mar;23(3):323-30
4. Deichmann R, and Haase A. Quantification of T1 Values by SNAPSHOT-FLASH NMR Imaging. Journal of Magnetic Resonance. 1992; 96, 608-612
Figures