1749
Assessment of chronic hepatitis B liver fibrosis staging using Intravoxel incoherent motion MRI compared with ultrasonic transient elastography1Tianjin First Center Hospital, Tianjin, China, 2Philips healthcare, Beijing China, Beijing, China
Synopsis
we compare the value of IVIM and ultrasonic transient elastography in evaluating the fibrosis staging of patients with chronic hepatitis B, and we found that IVIM is potential to assese chronic hepatitis B liver fibrosis and inferior to ultrasonic transient elastography, however Dslow and f have comparable diagnostic value with ultrasonic transient elastography in evaluating in liver fibrosis stage≥F3.
purpose
Liver fibrosis is a common pathological change of various chronic liver diseases, endangering human health. During the formation of liver fibrosis[1,2], abnormal deposition of extracellular matrix affects the diffusion direction, diffusion degree and hepatic sinus pressure of water molecules in the tissue,and all of above cause the change of liver stiffiness. Then Intravoxel incoherent motion (IVIM) imaging uses a double exponential model[3], which can measure the diffusion characteristics of water molecules in the random motion of tissues and the microcirculation perfusion information of blood flowing in capillaries. Recently, ultrasonic transient elastography using FibroScan, which is a rapid, noninvasive, and reproducible method[4,5], has been demonstrated to be a reliable tool for assessing liver fibrosis and cirrhosis. So the purpose of this research is to compare the dignostic performance of Intravoxel incoherent motion MRI comparied with ultrasonic transient elastography in staging liver fibrosis of chronic hepatitis B.Materials and Methods
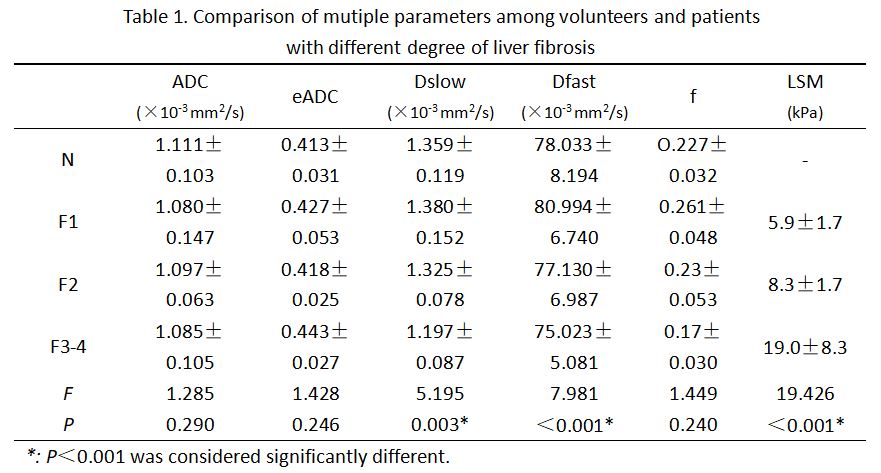
37 patients with chronic hepatitis B, including 14 patients( 5 femals, 9men; average age: 35.6±5.7y, range age: 24-58 ) with liver fibrosis stage F1, 14 patients ( 5 femals, 9men; average age: 35.6±5.7y, range age: 27-45 ) with F2, and 9 ( 7 femals, 2men; average age: 35.6±14.7y )with F3-4 confirmed by liver biopsy, and 16 normal volunteers (named N) were collected in this study. All subjects underwent Intravoxel incoherent motion MRI (IVIM MRI) scan and all patients underwent ultrasonic transient elastography examination. Mutiple parameters including apparent diffusion coefficient (ADC), exponential apparent diffusion coefficient (eADC) and pure diffusion (Dslow), perfusion-related diffusion (Dfast), perfusion fraction (f) (obtained by IVIM mono-exponential and bi-exponential models, respectively), and liver stiffness measurement (LSM) were comparied in different liver fibrosis staging and normal volunteers. Multiple parameters were correlated with liver fibrosis staging, and ROC was used to evaluate the diagnositic efficacy of above parameters in assesing liver fibrosis stagingResults
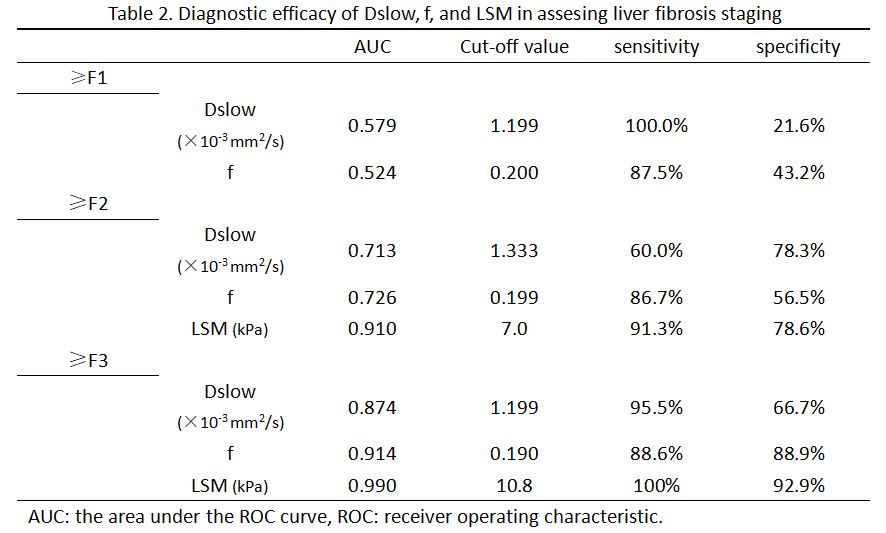
Dslow, f and LSM existed significant difference among different liver fibrosis staging and normal volunteers (P=0.03, P<0.001, and P<0.001), Dslow and f of N vs. F3-4, F1 vs. F3-4, and F2 vs. F3-4 were significantly different (all P<0.05), f of N vs. F1, N vs. F3-4, was significantly different (P=0.032), LSM of F1 vs. F3-4, and F2 vs. F3-4 had significant difference (P<0.001, and P<0.001). Dslow and f showed negetive relationship with liver fibrosis staging ( r=-0.557, P<0.001; r=-0.638, P<0.001 ), LSM was positive related with liver fibrosis staging ( r=0.827, P<0.001). AUC of Dslow, f, and LSM in assesing liver fibrosis stage ≥F3 and LSM in assesing liver fibrosis stage ≥F2 were all more than 0.87, sensitivity was ranged from 88.6% to 100%, and specificity was ranged from 66.7% to 92.9%. AUC of Dslow and f in assesing liver fibrosis stage ≥F2 were both more than 0.71, sensitivity was 60.0% and 86.7%, and specificity was 78.3% and 56.5%, respectively.Conclusion
IVIM MR is potential to assese chronic hepatitis B liver fibrosis and inferior to ultrasonic transient elastography, however Dslow and f have comparable diagnostic value with ultrasonic transient elastography in evaluating in liver fibrosis stage≥F3.Acknowledgements
No acknowledgement found.References
1. Wallace K, Burt AD, Wright MC. Liver fibrosis. Biochem J, 2008;411:1-18.
2. Su TH, Kao JH, Liu CJ. Molecular mechanism and treatment of viral hepatitis-related liver fibrosis. Int J Mol Sci 2014;15:10578-10604.
3. B. Le, D. ihan, E. Breton, D. Lallemand, P. Grenier, E. Cabanis, M. Laval-Jeantet, MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders, Radiology 161 (1986) 401–407.
4. Castera L, Vergniol J, Foucher J, et al. Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology. 2005;128:343-350.
5. Ziol M, Handra-Luca A, Kettaneh A, et al. Noninvasive assessment of liver fibrosis by measurement of stiffness in patients with chronic hepatitis C. Hepatology. 2005;41:48-54.
Figures