1746
Alteration of blood flow in hepatic fibrosis: preliminary resultsJeongHee Yoon1, Jeong Min Lee1,2, Moon Jung Hwang3, Hiroyuki Kabasawa4, and Joon Koo Han1
1Seoul National University Hospital, Seoul, Korea, Republic of, 2Seoul National University college of medicine, Seoul, Korea, Republic of, 3GE Healthcare, Seoul, Korea, Republic of, 4GE Healthcare, Tokyo, Japan
Synopsis
Portal flow is believed to relate to liver regeneration and may reflect the hemodynamic change of liver cirrhosis. So far, it has been relied on Doppler examination, which only sampled in local two-dimensional (2D) acquisition planes. Recently, four-dimensional (4D) flow acquisition of MRI may provide more accurate vascular flow information. However, there have been only a few studies of the liver in the literature.
Introduction
Portal flow is believed to relate to liver regeneration, but its exact mechanism has not been completely elucidated yet. In a preclinical study, portal overflow has been responsible to postoperative liver failure as well as hampered liver regeneration (1). Thus, preoperative portal flow measurement might be clinically valuable. The information has been provided by using Doppler ultrasound, however, it is highly operator dependent and only sampled in local 2D acquisition planes. MRI technique including 2D cine phase contrast MRI has been reported to show less intra- or inter-observer variability compared to Doppler US, but also limited to 2D plane acquisition. Recently, 4D flow acquisition has been drawing a lot of attention, since it may provide more accurate vascular flow information by 3D volume acquisition. However, there have been only a few studies in the literature (2-4), probably due to relatively new application to the liver and technical complexity. Thus, the purpose of this study is to investigate the technical feasibility of 4D flow in the liver, and the correlation between hepatic fibrosis stage and portal flow.Methods
This IRB-approved prospective ongoing study has enrolled 15 participants who met following eligibility criteria: a) chronic liver disease patients; b) or transplantation recipient on anti-viral medication; AND c) scheduled for liver resection, biopsy or transient elastography; AND d) sign informed consent. Participants underwent liver dynamic contrast-enhanced MRI including 4D flow sequence at 3T (Discovery 750w, GE Healthcare, Milwakee, USA) using a 36-ch phase-array body coil. The whole abdomen was scanned with coronal plane to cover the portal vein, splenic vein, and superior mesenteric vein (SMV). Scan parameters were as follows: FOV=380x380 mm2, matrix 180x180, slice thickness 3.0mm, TE=2.8ms, TR=11.6 ms, flip angle = 8, bandwidth= 62.5KHz, velocity sensitivity = 30 cm/s, and reconstructed spatial resolution 1.56 x1.50 x 1.56 mm3, and the slice number differed per subject volume. The average scan time of 4D flow sequence was 8~12min. Flow was measured in main portal vein, superior mesenteric vein, and splenic vein at least 1cm distance from the mesosplenic confluence and portal vein at hilar portion, using dedicated web-based software (ARTERYSTM, USA) (Figure 1). Flow of each vessel and difference of flow between vessels were compared between F0-2 and F3-4 (advanced fibrosis).Results
After excluding two participants whose raw data was failed to be stored, 4D flow data of 13 participants (M:F =10:3, mean age 59.7±7.6 years) were included for analysis. Median interval between 4D flow MRI and biopsy (n=3) or surgery (n=10) was 1 day (range: 0-8 days). Fibrosis grades were as follows: F0 (n=1), F1 (n=3), F2 (n=2), F3 (n=2), and F4 (n=5). Main portal vein flow significantly decreased (4.6±1.5 ml/sec vs. 7.4±2.5 ml/sec, P=0.025) in advanced hepatic fibrosis (F3-4) compared with F0-2. Intrahepatic portal flow which was measured at portal hilum decreased in advanced fibrosis (2.5±1.4 ml/sec vs. 4.2±2.8 ml/sec) but did not reach the statistical significance (P=0.2). In advanced fibrosis, flow at splenic vein (1.9±1.0 ml/sec vs. 2.1±1.0ml/sec) and SMV (2.7±1.1 vs. 3.9±1.8 ml/sec) did not show a significant difference from F0-2. The difference between main portal vein and splenic vein was significantly higher in F0-2 than F3-4 (5.3±2.4 ml/sec vs. 2.6±1.0 ml/sec, P=0.02). The difference between main portal vein and SMV was also higher in F0-2 (3.9±1.8 ml/sec vs. 2.7±1.1 ml/sec, P= 0.03). Mean areas of measurement were 0.6±0.8cm2 for intrahepatic portal vein, 0.7±0.3cm2 for main portal vein, 0.4±0.1cm2 for SMV, and 0.2±0.1cm2 for splenic vein.Conclusion
Our study revealed that portosystemic vascular flow is measurable on MRI using 4D flow sequence in acceptable time frame. Main portal vein flow decreased in advanced fibrosis compared with those without advanced fibrosis whereas splanchnic flow and splenic flow was less affected. Further studies with large population is needed.Acknowledgements
No acknowledgement found.References
1. Wang X, Xu Y, Tan J et al. Portal inflow preservation during portal diversion in small-for-size syndrome. WJG 2014;20(4):1021-1029 2. Stankovic Z, Rossle M, Euringer W et al, Normal and Altered Three-dimensional Portal Venous Hemodynamics in Patients with Liver Cirrhosis. Radiology 2012, 262(3):862-873 3. Roldan-Alzate A et al, Impaired regulation of portal venous flow in response to a meal challenge as quantified by 4D flow MRI. JMRI 2015;42(4):1009-17 4. Roldan-Alzate A et al, In vivo validation of 4D flow MRI for assessing the hemodynamics of portal hypertension. JMRI 2013;37(5):1100-1108Figures
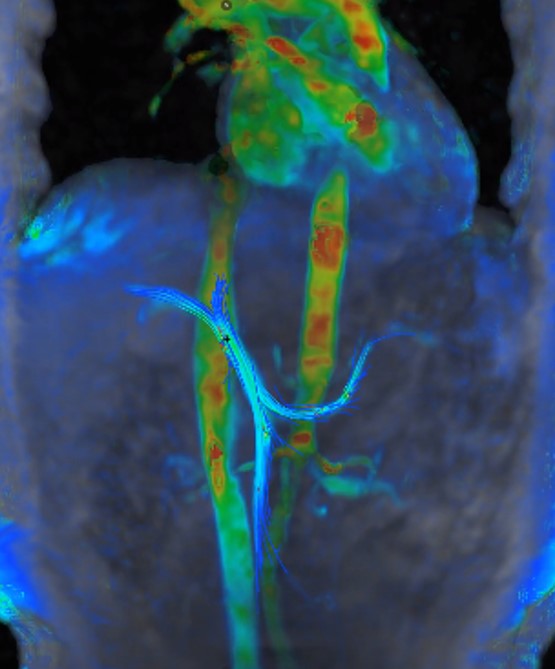
Fig 1.
A 62-year old woman with chronic hepatitis B. Four-dimensional (4D) flow MR
image with streamline reconstruction visualizes flow in main portal vein,
superior mesenteric vein, and splenic vein.