1737
Evaluation of Fontan Associated Liver Disease (FALD) with MRI: Does cardiac function play a role?1Radiology, University of Wisconsin - Madison, MADISON, WI, United States, 2Radiology, Medical Physics, Biomedical Engineering, Medicine, Emergency Medicine, University of Wisconsin - Madison, MADISON, WI, United States
Synopsis
The Fontan procedure prolongs survival in patients with congenital heart disease with mono-ventricle physiology but is associated with multiple long-term complications, including Fontan associated liver disease (FALD). The pathophysiology of FALD is poorly understood. In this study, the relationship between ventricular ejection fraction (EF) and FALD was investigated through a retrospective review of 24 Fontan patients who underwent cardiac and liver MRI. No correlation was identified between systemic ventricular EF and liver stiffness. This demonstrates the need for further investigation into the pathophysiology of FALD. Potential exploration may include flow related differences, or variations in systemic venous pressures.
Introduction
The Fontan procedure has helped alleviate many cardiac complications arising in patients with congenital heart disease and single ventricle physiology. This palliative procedure has resulted in significantly prolonged survival. However, as patients with Fontan survive longer, they face a multitude of extra-cardiac complications. Fontan associated liver disease (FALD) is universal among Fontan patients, and increases in severity with increasing time from surgery1. The pathophysiology of this process is poorly understood, and the severity of FALD ranges from mild fibrosis to cirrhosis and HCC2. Evaluation of the extent of liver fibrosis with biopsy is invasive and is limited by sampling variability3. Magnetic resonance elastography (MRE) measures the stiffness of liver parenchyma, which has been shown to be accurate for staging of liver fibrosis4. The purpose of this work is to evaluate the relationship between liver stiffness, as a surrogate biomarker of liver fibrosis, with ventricular function.Methods
We performed a retrospective review of cardiac MRI and/or MRE done in Fontan patients according to an IRB-approved and HIPAA-compliant protocol. A total of 24 patients, with imaging acquired between January 2015 and October 2018 met these criteria. Images and reports were reviewed and the ventricular EF, liver stiffness, liver proton density fat fraction (PDFF), type of ventricle, date of procedure, age and sex of the patient were recorded. Pearson correlation coefficients, T-tests and P-values were calculated to assess relationship between these parameters.Results
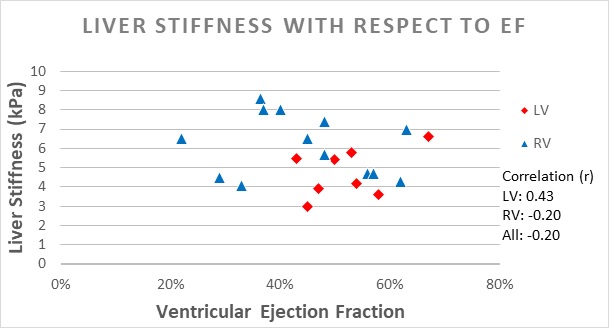
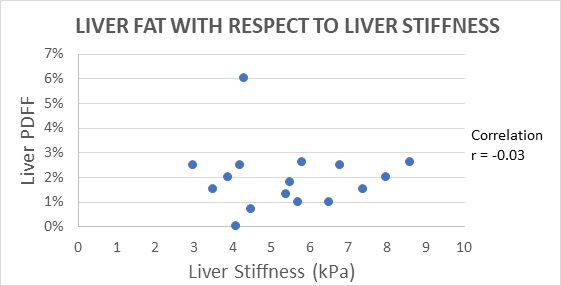
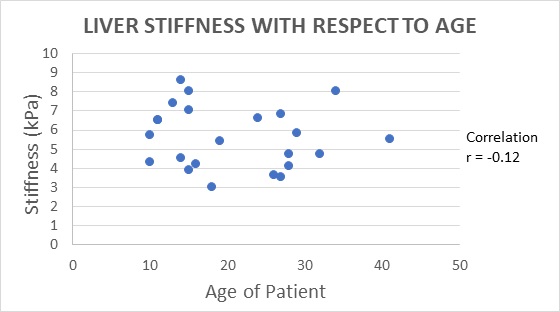
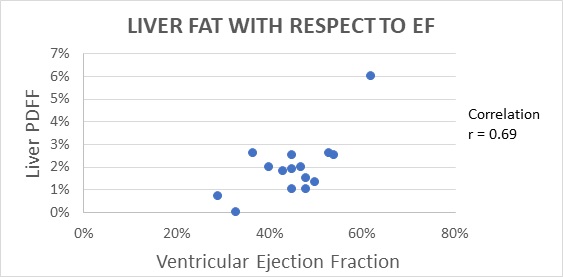
The data demonstrated an average age of 21 years (min 10, max 40, SD of 9). There was a total of 11 females and 13 males. 15 of the patients had a morphologic right ventricle, while 9 of the patients had a morphologic left ventricle. The mean values for EF, liver stiffness, and PDFF were 47% (min 22%, max 67%, SD of 11%), 5.56 kPa (min 3, max 8.6, SD 1.6), and 2.0% (min 0.0%, max 6.0%, SD 1.3%), respectively. No correlation was identified between ventricular EF and liver stiffness in 21 patients that had both cardiac MRI and MRE (r = -0.20, p = 0.39). There was also no correlation between liver stiffness and liver PDFF (r = -0.03, p = 0.92) or liver stiffness and the age of the patient (r = -0.12, p = 0.58). Interestingly, there was a mild positive correlation between liver PDFF and ventricular EF (r = 0.69, p=0.01). There was a slight trend towards increased liver stiffness in patients with a morphologic RV (mean stiffness = 5.96 kPa) when compared to a morphologic LV (mean stiffness = 4.98 kPa), however it was not statistically significant (p=0.15).Discussion
In this work, we evaluated liver stiffness, as a surrogate for liver fibrosis, and its relationship to ventricular function in patients with Fontan circulation. Intuitively, one would expect this correlation to exist because if ventricular function decreases, there would presumably be increased hepatic congestion, which would lead to increased stiffness5,6. In our patient population, a correlation between liver stiffness and ventricular function was not observed.
Further, the lack of correlation between liver PDFF and liver stiffness demonstrates that this process is unlikely related to increased fat accumulation and/or non-alcoholic steatohepatitis.Furthermore, the lack of correlation between age and liver stiffness indicates that this process is unlikely related to other age-related factors. A slight trend of positive correlation between PDFF and ventricular function may be related to overall increased energy absorption and storage in patients with better cardiovascular efficiency. Patient’s that had a right ventricle showed a slight trend toward having increased liver stiffness. Because lower ventricular function was not correlated to increased liver stiffness, there are likely additional differences between the right and left ventricle which are contributing to this difference. This may be related to flow related differences, or other physiologic differences that have not been monitored or uncovered.
Conclusion:
Unexpectedly, no correlation between liver stiffness and ventricular function was observed in patients with mono-ventricular physiology and Fontan repair. Further evaluation of the pathophysiology of liver disease in Fontan patients is warranted. Potential areas of exploration include flow related differences between the patients, and differences in systemic venous pressures, which may contribute to varying degrees of liver damage. Additional insight into this area can provide improved monitoring, care and overall survival in these patients.Acknowledgements
No acknowledgement found.References
References:
1) Wu FM, Kogon B, Earing MG, Aboulhosn JA, Broberg CS, John AS, et al. Liver health in adults with Fontan circulation: a multicenter cross-sectional study. J Thorac Cardiovasc Surg 2017; 153:656-664.
2) Romero R. Liver in congenital heart disease: implications of the fontan procedure for pediatric and adult liver specialists. Clin Liver Dis 2013;2:210-214.
3) Ratziu V, Charlotte F, Heurtier A, Gombert S, Giral P, Bruckert E, Grimaldi A, Capron F, Poynard T; Sampling variability of liver biopsy in nonalcoholic fatty liver disease. Gastroenterology. 2005 Jun;128(7):1898-906.
4) Morisaka H, Motosugi U, Ichikawa S, Nakazawa T, Kondo T, Funayama S, Matsuda M, Ichikawa T, Onishi H. Magnetic resonance elastography is as accurate as liver biopsy for liver fibrosis staging. J Magn Reson Imaging. 2018 May;47(5):1268-1275.
5) Bryant T, Ahmad Z, Millward-Sadler H, Burney K, Stedman B, Kendall T, Vettukattil J, Haw M, Salmon AP, Cope R, Hacking N, Breen D, Sheron N, Veldtman GR. Arterialised hepatic nodules in the Fontan circulation: hepatico-cardiac interactions. Int J Cardiol. 2011 Sep 15;151(3):268-72.
6) Diamond, T. and Ovchinsky, N. (2018), Fontan‐associated liver disease: Monitoring progression of liver fibrosis. Clinical Liver Disease, 11: 1-5.
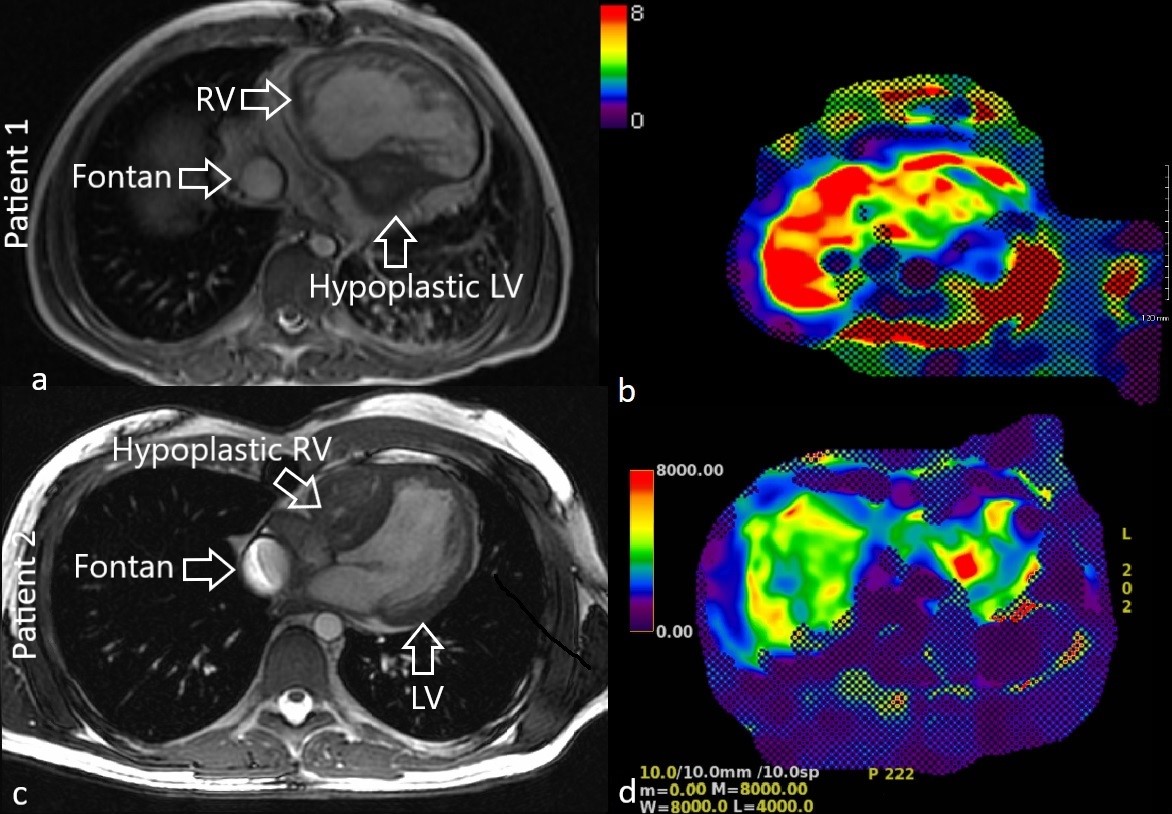
Figures