1717
Evaluation of Variable-TE computed Diffusion Weighted Imaging Technique using Deep Learning based Noise Reduction1MRI development department, Canon Medical Systems Corporation, Tochigi, Japan
Synopsis
In this study to the authors adapted the variable-TE cDWI(vTE-cDWI) technique applying denoise approach with deep learning reconstruction(dDLR) to the abdominal region, using ADC-map, T2-map and T1-map with IR-based images. The algorithm under evaluation allows computing diffusion images for arbitrary combinations of TE, b-value and TI based on four acquisitions(4-points method). This technique was shown to generate vTE-cDWI with higher SNR compared to the acquired DWI, and dDLR increased the SNR more, as well as obtain ADC-maps and T1-maps with optimal TI for any arbitrary tissue. The clinical benefits of the method and results on volunteers are discussed.
PURPOSE:
A computed diffusion weighted imaging(cDWI) was previously presented, demonstrating improvement in lesion detection[1-3]. This algorithm works by computing high b-value-equivalent(b) images from relatively low-b images. Recently a variable-TE cDWI(vTE-cDWI) technique was proposed for the brain allowing the computation of DWIs with arbitrary combinations of TE and b[4]. This method can control the T2-shine-through effects and optimize the SNR and CNR of tissues. However, for creating higher b value images with higher accuracy, the original image with higher SNR is necessary.
Noise reduction technique is one of the methods to solve this problem. We have developed the denoise approach with deep learning reconstruction(dDLR), as noise reduction technique based on deep learning, using high SNR images and images with various intensities of noise added[5][6].
In this study we extended the vTE-cDWI technique, applying dDLR to each map images(T1,T2,ADC), adapting it to the abdomen[7]. Improved CNR and SNR is achieved by computing images with arbitrary TE and b, while reducing the T2-shine-through effects and allowing for selective tissue suppression through the arbitrary TI.
METHODS:
Theory: For a SEEPI2D(mDWI) with set TE and b, the intensity at voxel location characterized by known T2 and ADC parameters is described by:
S(TE,b)=k⋅exp((−TE)/T2)⋅exp(−b⋅ADC)⋅⋅⋅(1)
k being a constant for the voxel. Similarly, IR-based mDWI signal intensity at given TI, TE, and b when TR is set to infinity is described by:
S(TI,TE,b)=k⋅(1−2exp(−TI/T1))⋅exp(−TE/T2)⋅exp(−b⋅ADC)⋅⋅⋅(2)
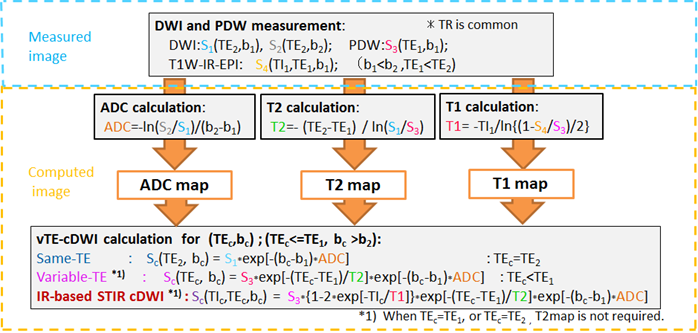
A 4-point cDWI method was applied, along the algorithm shown in Fig.1, as follows:
a)Same-TE cDWI[1-3]:
A 2-points technique is applied, measuring mDWI signals at the same TE=TE2 for two different b-values (b1<b2), and solving (1) for the ADC:
ADC=−ln[S2(TE2,b2)/S1(TE2,b1)]/(b2−b1).⋅⋅⋅(3)
The cDWI image at the original TE=TE2 and for arbitrary b=bc is obtained by replacing (3) into (1):
Sc(TE2,bc)=S1(TE2,b1)⋅exp[−(bc−b1)⋅ADC].⋅⋅⋅(4)
B)Different-TE cDWI (vTE-cDWI)[4]:
The tissue T2 can be obtained from (1) by measuring two mDWI with the same b=b1 and different TEs (TE1<TE2):
1/T2=−ln[S1(TE2,b1)/S3(TE1,b1)]/(TE2−TE1).⋅⋅⋅(5)
The diffusion image at arbitrary TE=TEc and b=bc is obtained replacing the calculated ADC (3) and T2 (5) in (1):
Sc(TEc,bc)=S3(TE1,b1)⋅exp[−(TEc−TE1)/T2]⋅exp[−(bc−b1)⋅ADC].⋅⋅⋅(6)
(6) allows to compute sTE-cDWI images free of T2-effects(TEc=0).
C)IR-based STIR vTE-cDWI:
T1 is derived from (2) with the IR term in S4(TI1,TE1,b1) by setting TI=TI1, the SE signal of PDW S3(TE1,b2), and selecting a sufficiently long TR2:
1/T1=(−ln[(1−S4/S3)/2])/TI1⋅⋅⋅(7)
By replacing the calculated ADC (3), T2 (5), and T1 (7) in (2), we can compute the diffusion image at arbitrary TI=TIc, TE=TEc and b=bc as:
Sc(TIc,TEc,bc)=S3⋅[1−2⋅exp(−TIc/T1)]⋅exp[−(TEc−TE1)/T2]⋅exp[−(bc−b1)⋅ADC].⋅⋅⋅(8)
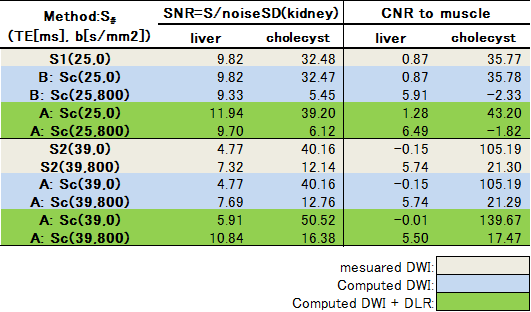
Volunteers study: The models described above were validated on three volunteers. Abdominal axial scans through the liver were acquired on a Canon 3T MR system using a single-shot SEEPI2D sequence. Acquisition parameters for the 4-points mDWI scans were: TE1=25ms, b1=0 without inversion and TE1=25ms, b1=0 with TI1=600ms, TE2=39ms with b1=0 and b2=800s/mm2. TE3=45ms and TE4=60ms with b1=0 were also acquired for a more accurate assessment of the T2 map. The T1 map was calculated with TI-off(=infinity) and TI=600ms for the same TE1=25ms. The cDWI and STIR-cDWI signals for bc=800, and 1500s/mm2 were calculated at different TEc. In addition, dDLR was applied to each map, and same cDWI and STIR-cDWI images were calculated at the image after adaptation. ROIs were drawn on the liver, cholecyst, kidney, and the erector spinae muscle. SNR related to kidney-SD and CNR with respect to the muscle were measured for each ROI(Table.1).
RESULTS AND DISCUSSION:
Volunteers’ scans demonstrated an increased liver-to-muscle CNR for shorter TEs, suggesting that the cDWI can improve the characterization of tissues with short T2. SNRs in dDLR image for vTE-cDWI increased at all condition compared to mDWI and vTE-cDWI without dDLR(Fig.2). The shoter-TE cDWI with dDLR has a PDwi contrast, therefore a decreased signal for (TE, b)=(25, 800) is descriptive of the diffusion properties with higher SNR and less T2 shine-thorough effects.
SNRs in the liver and cholecyst for the IR-based STIR vTE-cDWI(method-C) increased at (TI1,TE,b)=(280,60,1500) compared to the STIR-mDWI. SNRs in dDLR image for STIR vTE-cDWI also increased at all condition compared to without dDLR. The IR-based STIR vTE-cDWI with dDLR in the abdomen is meant for fat suppression or background suppression, and benefits from controlling TE, b and TI(Fig.3,Fig4). This technique demonstrated an improved CNR compared to acquired images because of the contribution of the T1 map.
CONCLUSION:
In this study the authors adapted the vTE-cDWI technique and dDLR technique to relevant cases of abdominal imaging. It was demonstrated that the both techniques are capable of generating vTE-cDWI and STIR-cDWI with higher SNR compared to acquired DWI, with the additional benefit of generating the ADC map and T1 map with an optimal TI for any predetermined tissue. The method may be expected to be clinically useful for improved characterization of liver masses through more efficient suppression of surrounding tissues.Acknowledgements
No acknowledgement found.References
[1] Blackledge MD, Leach MO, Collins DJ, et al. Computed Diffusion-weighted MR Imaging May Improve Tumor Detection. Radiology: 261,573-581(2011).
[2] Ueno Y, Takahashi S, Kitajima K, Kimura T et al. Computed diffusion-weighted imaging using 3-T magnetic resonance imaging for prostate cancer diagnosis. Eur Radiol 23,3509-16 (2013).
[3] Kimura T, Machi Y. Computed Diffusion Weighted Imaging Under Rician Noise Distribution. In: Proceedings of the 20th Annual Meeting of ISMRM, 2012;p3574.
[4] Kimura T, Machi Y et al. A short-TE Computed Diffusion Imaging (cDWI). In: Proceedings of the 23th Annual Meeting of ISMRM, 2015;p2929.
[5] K. Isogawa, T. Ida, T. Shiodera and T. Takeguchi, "Deep Shrinkage Convolutional Neural Network for Adaptive Noise Reduction," IEEE Signal Processing Letters, vol. 25, no. 2, pp. 224-228, 2018.
[6] K. Isogawa, T. Ida, T. Shiodera et al. Deep Convolutional Neural Network for Image Denoising. In: Proceedings of the 26th Annual Meeting of ISMRM, 2018;823.
[7] Warntjes JBM et al. Rapid Magnetic Resonance Quantification on the Brain. Magn Reson Med 60:320–329 (2008).
Figures