1705
The Diagnostic Performance of LI-RADS version 2018 and the Value of Ancillary Features Favoring Hepatocellular Carcinoma (HCC) in the Diagnosis of 10-19 mm HCC on Extracellular Contrast-enhanced MRI.1Department of Radiology, The third affiliated hospital of Sun Yat-sen University, guangzhou, China, 2Department of Radiology, University of California at San Diego, La Jolla, CA, United States
Synopsis
Hepatocellular carcinoma (HCC) is the second most cause of cancer death worldwide. Early detection of small HCC can prolong patient survival. Recent updates have changed diagnostic criteria for LI-RADS v2018 for 10-19 mm HCC, and the impact on accuracy has not yet been studied. We found that LI-RADS v2018 provides 68.2% sensitivity, 91.7% specificity, and 71.8% accuracy for 10-19 mm HCC diagnosis in a Chinese population with chronic liver disease. Several modifications of LI-RADS were explored (e.g., pooling LR-4 and LR-5; allowing ancillary features favoring HCC to upgrade LR-4 to LR-5 and/or convert LR-M to LR-5), some sensitivities were mild improved without specificities increase.
Introduction
Hepatocellular carcinoma (HCC) is the second most common cause of cancer death worldwide1. Early detection of < 20-mm HCC can prolong patient survival2. Unlike other malignancies that require tissue diagnosis, HCC is diagnosed noninvasively by imaging-based criteria without confirmatory biopsy3, 4. The Liver Imaging Reporting and Data System (LI-RADS) standardizes liver imaging in patients at risk for HCC. As LI-RADS was primarily developed in the context of transplant allocation, it emphasizes specificity, and has shown only fair sensitivity for HCC despite several updates since it was first released in 20112, 5, 6. The most recent version of LI-RADS, v2018, attempts to improve sensitivity by reducing the stringency for 10-19 mm HCC7. However, the diagnostic performance and impact on specificity of these revised LI-RADS v2018 criteria for 10-19 mm HCC have not yet been studied. The purpose of this study was to evaluate the diagnostic performance of LI-RADS v2018 for 10-19 mm HCC and to explore whether modifications to LI-RADS could further improve sensitivity without reducing specificity.Methods
Our institutional review board approved this retrospective cohort study with waived informed consent requirement. We identified all patients with chronic liver disease with one to three 10-19 mm observations reported clinically on a 1.5T or 3.0T extracellular contrast agent-enhanced (ECA-) MRI exam in our hospital from May 2004 to May 2018. Patients were excluded if they had liver surgery or locoregional therapy prior to MRI or if a rigorous reference standard could not be established. The reference standard was histopathology if the time interval between MRI and histopathology sampling was ≤ 30 days; otherwise, it was based on the composite of all available clinical and imaging data after a minimum of two years of follow up. Blinded to the reference standard classification, two abdominal radiologists, independently reviewed the MR images. All major features were recorded using LI-RADS v2108, except threshold growth or those requiring comparison to prior exams7. A final LI-RADS v2018 category was assigned with major features. Discordance was resolved by consensus. Observations were then recategorized according to LI-RADS v2018 or several modified version of LI-RADSs. These modified versions included pooling LR-4 and LR-5, allowing ancillary features favoring HCC7(AFs-HCC) to upgrade LR-4 to LR-5, allowing AFs-HCC to convert LR-M to LR-5, and every combination of the above. The diagnostic sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) of LR-5 and of each modified LR-5 were determined and compared.Results
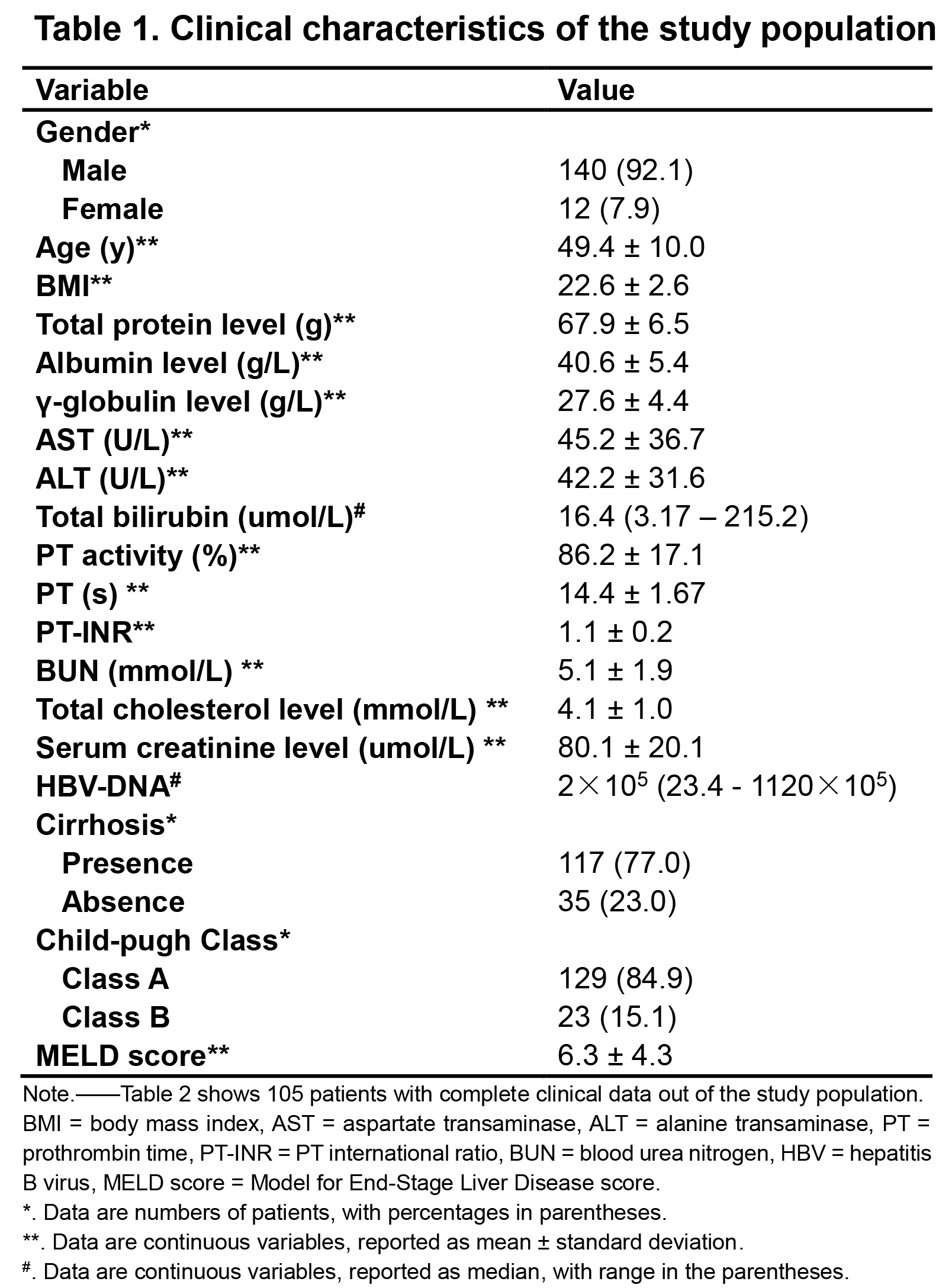
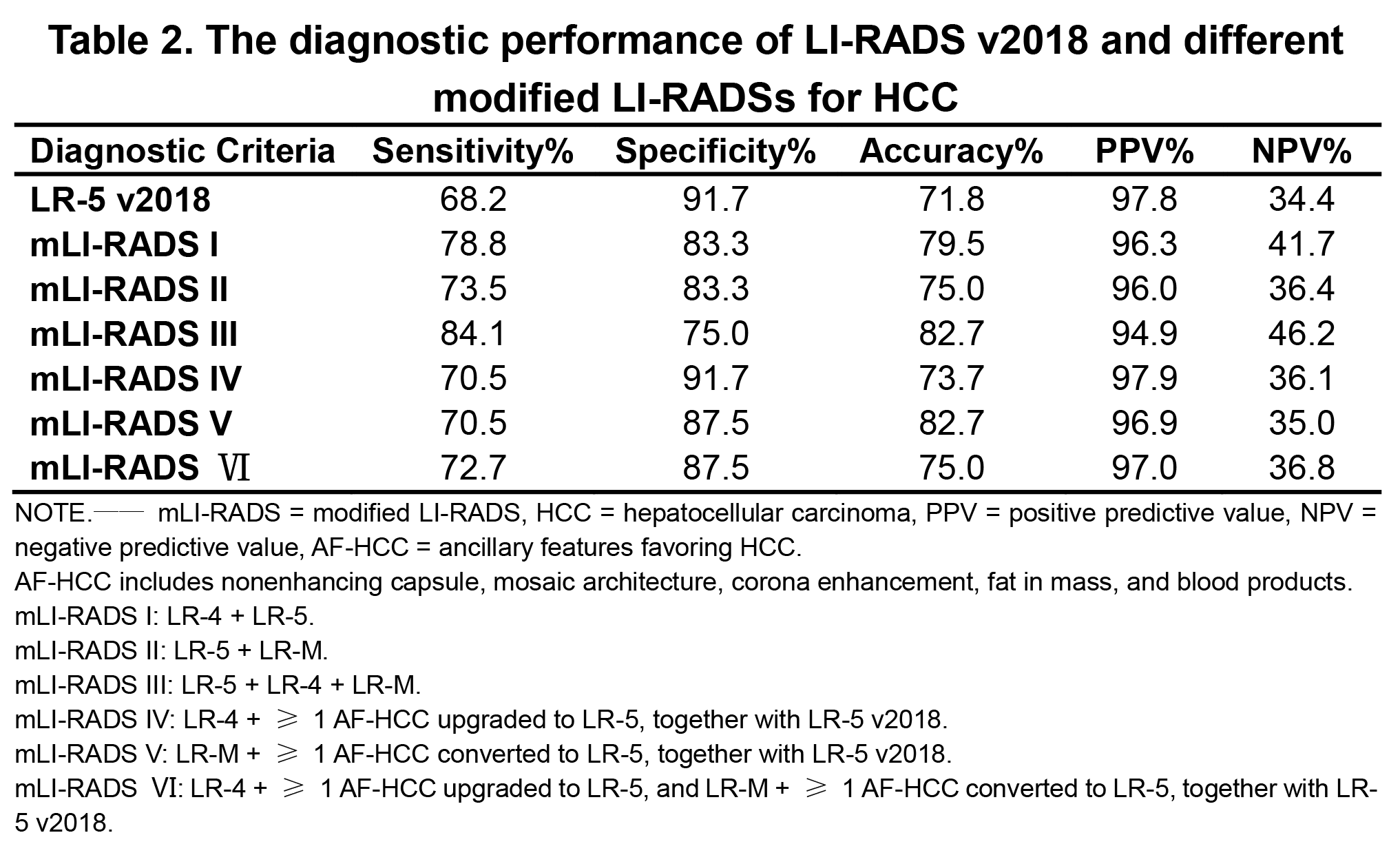
152 patients with chronic liver disease and with a total of 156 one to three 10-19 mm observations. Table 1 summarizes clinical characteristics. Of the 156 observations, there were 132 (84.6%) HCCs, 3 (1.9%) iCCAs, 2 (1.3%) cHCC-CCAs, 1 (0.6%)dysplastic nodule, 2 (1.3%) hepatocellular adenomas, 4 (2.6%) focal nodular hyperplasias, 4 (2.6%) hemangiomas, 7 (4.5%) perfusion alterations, and 1 (0.6%) inflammatory scarring. Overall, 0% LR-1 (0/3) and LR-2 (0/8), 75.0% (21/28) LR-3, 87.5% (14/16) LR-4, 97.8% (90/92) LR-5, and 77.8% (7/9) LR-M were HCC according to standard LI-RADS v2018. The sensitivity, specificity, accuracy, PPV, and NPV of LR-5 in LI-RADS v2018 and different mLI-RADSs criteria for diagnosis of HCC are shown in table 2. The accuracy of LR-5 as defined by LI-RADS 2018 for 10-19 mm HCC was modest with a sensitivity, specificity, and accuracy of 68.2%, 91.7%, and 71.8%, respectively, Among the diagnostic criteria for HCC, mLI-RADS IV showed slightly higher sensitivities (70.5% vs. 68.2%) and accuracy (73.7% vs. 71.8%) than LI-RADS v2018 with maintained high specificity (91.7% vs. 91.7%). mLI-RADS III or mLI-RADS V showed the highest accuracies of 82.7% but in the expense of decreased in sensitivity or specificity.Discussion
In our study, the accuracy of LR-5 as defined by LI-RADS 2018 for 10-19 mm HCC was modest with a sensitivity, specificity, and accuracy of 68.2%, 91.7%, and 71.8%, respectively, which were similar to those in LI-RADS v20172.We found that the modified versions of LI-RADS incorporating different combinations of ancillary features yielded increased sensitivity but did not increase the specificity of LR-5 for HCC. Several limitations bear mentioning, such as the single-center, retrospective design, which probably resulted in selection bias for higher LI-RADS categories and verification bias for malignant lesions. The prevalence of cirrhosis and of Child-Pugh > A cirrhosis was low, limiting generalizability to Western populations. HBP imaging features were not examined.Conclusion
The diagnostic accuracy of LR-5 as defined by LI-RADS v2018 for 10-19 mm HCC was modest using ECA-MRI in a Chinese population with chronic liver disease. Modifications to LI-RADS can increase the sensitivity butnot improve the specificity.Acknowledgements
The authors state that this study has received funding by National Natural Science Foundation of China grant 81271562 (JW) and Science and Technology Program of Guangzhou, China 201704020016 (JW).References
1. Bertuccio P, Turati F, Carioli G, et al. Global trends and predictions in hepatocellular carcinoma mortality. J Hepatol. 2017 Aug;67(2):302-309.
2. Ronot M, Fouque O, Esvan M, et al. Comparison of the accuracy of AASLD and LI-RADS criteria for the non-invasive diagnosis of HCC smaller than 3 cm. J Hepatol. 2017 Dec 21. pii: S0168-8278(17)32529-1.
3. European Association for Study of Liver; European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. Eur J Cancer. 2012 Mar;48(5):599-641.
4. Bruix J, Sherman M, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011 Mar;53(3):1020-2.
5. Alhasan A, Cerny M, Olivié D, et al. LI-RADS for CT diagnosis of hepatocellular carcinoma: performance of major and ancillary features. Abdom Radiol (NY). 2018 Aug 30. doi: 10.1007/s00261-018-1762-2.
6. Kierans AS, Makkar J, Guniganti P, et al. Validation of Liver Imaging Reporting and Data System 2017 (LI-RADS) Criteria for Imaging Diagnosis of Hepatocellular Carcinoma. J Magn Reson Imaging. 2018 Sep 26. doi: 10.1002/jmri.26329.
7. American College of Radiology. Liver imaging reporting and data system version 2018. http://www.acr.org/quality-safety/resources/LIRADS.
Figures