1698
Comparison of MR elastography and intravoxel incoherent motion for the prediction of hepatocellular carcinoma tumor capsule formation in hepatitis B virus-related patients using whole-tumor analysis1Department of Radiology, The third affiliated hospital of Sun Yat-sen University, Guangzhou, China, 2MR Research China, GE Healthcare, Beijing, China, 3Department of Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
Hepatocellular carcinoma (HCC) is the most common primary malignant hepatic tumor worldwide and the prognosis remains poor. Tumor capsule formation is a favorable factor for predicting invasiveness and prognosis. We explored the potential value of MR elastography(MRE)and intravoxel incoherent motion(IVIM)for the prediction of tumor capsule formation in patients with hepatitis B virus-related (HBV) HCCs using whole-tumor analysis. Results showed that mean tumor stiffness may be useful for the prediction of capsule formation of HCCs. The utility of the mean value of IVIM metrics may need to be further explored.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary malignant hepatic tumor worldwide and the third most common cause of cancer-related death[1, 2]. Despite the improvements in the treatment and postoperative management of HCC, the tumor recurrence rate remains high and the prognosis is still poor[3]. Encapsulated HCCs tend to have a lower incidence of direct liver invasion, fewer tumor microsatellites, less vascular invasion and better prognosis than nonencapsulated HCCs[4-6]. Therefore, preoperative diagnosis of capsule formation could be useful for choosing better treatments for patients with HCCs. MR elastography (MRE) is a noninvasive technique for the quantitative measurement of tissue stiffness[7, 8]. Intravoxel incoherent motion (IVIM) is an advanced imaging technique which allows for the simultaneous measurement of the diffusion of water molecules and the microcirculation of tissue without application of a contrast medium[9, 10]. The aim of this research was to compare the performance of MRE and IVIM for predicting the capsule formation of HCCs using whole-tumor analysis.
Methods
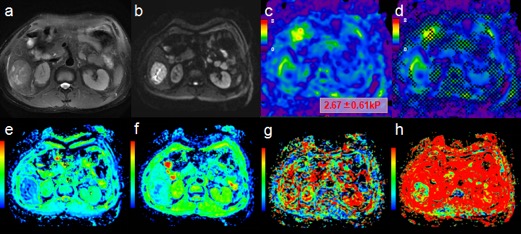
A total of 163 patients were recruited from December 2014 to August 2017 at our institute who were infected with the hepatitis B virus. The exclusion criteria were as follows: (a) the lesions were less than 3 cm in diameter; (b) the MRE image quality was inadequate; (c) the IVIM images had respiratory artifacts; (d) the time interval between surgery and the MR examination was more than one month; (e) previous transarterial chemoembolization (TACE) or radiofrequency ablation (RFA). 70 patients (63 males, 7 females; mean age: 49.18 years; range: 22-72 years) were included in the final cohort. Patients were classified into the encapsulated or nonencapsulated group. All patients were imaged using a 3.0T whole-body MR scanner (Discovery MR750, GE Healthcare, Milwaukee, WI). MRE was performed with a multislice, spin-echo echo-planar imaging (SE-EPI) 3D-MRE sequence using 60-Hz vibrations (acquisition matrix: 80x80; TR/TE:1334/52ms; single shot; scan time: 1:04 min; FOV: 44.8 cm; number of slices: 20; slice thickness: 3mm). The MRE magnitude and phase images were processed using a direct-inversion (DI) algorithm to calculate the stiffness. Respiratory-triggered diffusion-weighted imaging (DWI) (acquisition matrix: 128x128; TR/TE: 9231/56 ms; single shot; scan time: 3:52 min; FOV: 38x30cm; number of slices: 33; slice thickness: 5mm) was performed using 11 b values (b=0, 30, 50, 100, 150, 200, 300, 500, 800, 1000, 1500 sec/mm2). Regions of interest (ROIs) were placed on every slice containing lesions in the magnitude images and apparent diffusion coefficient (ADC) and IVIM maps tracing the margin with T2-weighted images as a reference. A volume of interest (VOI) covering the whole tumor was obtained by merging all of the ROIs. The mean values for the stiffness, ADC and IVIM parameters(D, true diffusion coefficient; D*, pseudodiffusion coefficient; f, pseudodiffusion fraction) over the whole tumor were calculated. The tumor capsule was reviewed by an experienced hepatopathologist who was blinded to the clinical and laboratory results. Data were evaluated using the two-sample t test or Mann-Whitney U test.
Results
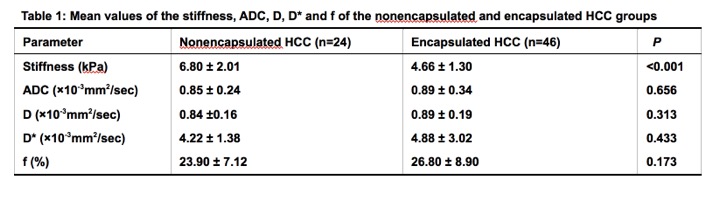
Among the 70 patients included in the study, 24 patients had tumor capsule and 46 patients did not have capsule. The mean values for the stiffness, ADC, D, D* and f of the nonencapsulated and encapsulated HCCs is shown in Table 1. The mean stiffness of nonencapsulated group was significantly higher than that of the encapsulated group (P˂0.001). On the other hand, the mean values for the ADC, D, D* and f were not significantly different between the two groups (P= 0.656, 0.313, 0.433 and 0.173, respectively).Discussion
Our preliminary results showed that the mean tumor stiffness was significantly higher in HCCs without tumor capsule compared to those with tumor capsule and that MRE has the potential to predict tumor encapsulation preoperatively. However, the mean values for the ADC and IVIM metrics of HCCs did not show any significant usefulness in predicting capsule formation using this whole-tumor analysis. The possible explanation might be that the diffusion and perfusion of tumors may have no correlation with the formation of the capsule. Further research is warranted to investigate the value of MRE and IVIM for predicting HCC capsule formation.Conclusion
The results of our study showed that MRE is a useful technique for predicting the formation of HCC capsules preoperatively using whole-tumor analysis. However, the value of ADC and IVIM metrics needs to be further investigated.Acknowledgements
The authors state that this study has received funding by National Natural Science Foundation of China grant 81271562 (JW) and Science and Technology Program of Guangzhou, China 201704020016 (JW).References
[1] Caldwell S, Park S H. The epidemiology of hepatocellular cancer: from the perspectives of public health problem to tumor biology. J Gastroenterol,2009,44 Suppl 19:96-101.
[2] Torre L A, Bray F, Siegel R L, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA: A Cancer Journal for Clinicians,2015,65(2):87-108.
[3] Wu J, Huang Y, Chau G, Su C, Lai C, Lee P, Huo T, Sheen I, Lee S, Lui W. Risk factors for early and late recurrence in hepatitis B-related hepatocellular carcinoma. Journal of Hepatology,2009,51(5):890-897.
[4] Encapsulation is a Significant Prognostic Factor for Better Outcome in Large Hepatocellular Carcinoma. Journal of Surgery Oncology,2011,105(1):85-90.
[5] Takeishi K, Maeda T, Shirabe K, Tsujita E, Yamashita Y, Harimoto N, Itoh S, Ikegami T, Yoshizumi T, Maehara Y. Clinicopathologic Features and Outcomes of Non-B, Non-C Hepatocellular Carcinoma After Hepatectomy. Annals of Surgical Oncology,2015,22(S3):1116-1124.
[6] Choi Y S, Rhee H, Choi J, Chung Y E, Park Y N, Kim K W, Kim M. Histological characteristics of small hepatocellular carcinomas showing atypical enhancement patterns on gadoxetic acid-enhanced MR imaging. Journal of Magnetic Resonance Imaging,2013,37(6):1384-1391.
[7] Pepin K M, Ehman R L, Mcgee K P. Magnetic resonance elastography (MRE) in cancer: Technique, analysis, and applications. Prog Nucl Magn Reson Spectrosc,2015,90-91:32-48.
[8] Venkatesh S K, Yin M, Glockner J F, Takahashi N, Araoz P A, Talwalkar J A, Ehman R L. MR elastography of liver tumors: preliminary results. AJR Am J Roentgenol,2008,190(6):1534-1540.
[9] Le Bihan D. Apparent diffusion coefficient and beyond: what diffusion MR imaging can tell us about tissue structure. Radiology,2013,268(2):318-322.
[10] Iima M, Le Bihan D. Clinical Intravoxel Incoherent Motion and Diffusion MR Imaging: Past, Present, and Future. Radiology,2016,278(1):13-32.
Figures